Page 1 of 6
6/29/2023
WELCOME TO OUR CLINIC! COVENANT HAND THERAPY, PC
Please take a few minutes to answer the following questions so we can better assist you with your health care and insurance needs.
P
ATIENT
’
S
N
AME
P
ATIENT
’
S
D
ATE OF
B
IRTH
P
RIMARY
I
NSURED
P
ERSON
&
I
NSURANCE
ID#
_
&
DOB_
&
E
MPLOYER
&
R
ELATIONSHIP TO PATIENT
I
NSURANCE
C
O
.
N
AME
I
NS
.
C
O
.
P
HONE
N
UMBER
P
LAN
G
ROUP
#
_P
LAN
E
FFECTIVE
D
ATE
circle: HMO POS PPO I WC
If
HMO
or
POS:
Primary
Care
Physician
(PCP)
Name
Phone
Is a PCP Referral Required? Yes No If yes, insurance referral obtained? Yes No
Referring/Prescribing
Doctor
Phone_
Patient’s
Diagnosis
:
This Benefit Verification form is only a potential explanation of coverage obtained from the patient’s insurance company & is
not a guarantee of coverage, eligibility or payment. If the information provided by the insurance company is not accurate or the
insurance company changes its coverage, the patient will be responsible for payment for services.
Patient Authorization, Release and Signature: I do not hold CHT &/or its affiliates responsible for any incorrect or omitted
information, or for any changes in my future coverage. I also agree that I am responsible for the contract between myself & my
insurance company.
Patient/Guardian
Signature
Date
CHT staff use:
Occupational & Physical THERAPIES, office setting
……
Pre-cert/auth?
Yes
No
Phone_
Deductible
$ _____
______
Notes
Portion
Met
to
Date
$
% Covered with Co-Pay Amount of % OR $ /visit
Out
of
Pocket
$
______
Portion
Met
to
Date
$
OT dollar limit $_
yr OT visit limit__
PT
dollar
limit
$
yr
PT
visit
limit_
Claim Requirements ______________________________
Ins.Rep.Name ________________
Calendar Year or Plan Year_
_____
______
Are S8950, 29581, 29582, 29583, 29584 covered?
Durable Medical Equipment / orthotics / garments
……
Pre-cert/auth?
Yes
No
Phone_
Deductible
$
________
Portion
Met
to
Date
$
...… if over $ .
% Covered with Co-Pay Amount of % or $ /visit
Out
of
Pocket
$
______
Portion
Met
to
Date
$
Dollar limit for DME $ yr. Item Limit _______________yr Splints… L3808… L3906… L3913 …L3933
Compression Garments
:
hose
…A6531…A6533…A6540
gloves
…A6504…S8425…S8427…S8428
ReadyWrap…
A6545
Farrow
…A6545
Circaid
…A4465
Abd binder
…L0625
Sleeves
…L8010…S8422…S8424
wraps
… S8429…S8430…S8431
Claim
Requirements
Ins.
Rep.
Name
Notes _________ ___________________
____________________________________________________________________________________________________________
____________________________________________________________________________________________________________
INS Call Ref#________________________________________________Verified by__________________Date/Time_____________

Page 2 of 6
6/29/2023
COVENANT HAND THERAPY, PC
1101 Ohio Drive, Suite 105, Plano, TX 75093 - phone 972-599-9594 - fax 972-599-9364
Patient Name
:
Patient’s Rights and Responsibilities
The patient has the right to considerate and respectful service. to obtain service without regard to race,
creed, national origin, sex, age, disability diagnosis or religious affiliation. (subject to applicable law) to
confidentiality of all information pertaining to his/her service. [Individuals or organizations not involved in the
patient’s care may not have access to the information without the patient’s written consent.] to make
informed decisions about his/her care. to reasonable continuity of care and service. to voice grievances
without fear of termination of service or other reprisal in the service process.
The patient is responsible for notifying CHT of any CHT DME equipment failure or damage. for any CHT
equipment that is lost or stolen while in their possession for notifying CHT of such loss. for notifying CHT of
any changes to their address or telephone. for notifying CHT of any changes concerning their physician. for
notifying CHT of discontinuance of use of issued CHT equipment. for any equipment rental and sale charges
which the patient’s insurance company does not pay, except where contrary to federal or state law.
HIPAA Privacy Policy Effective: 04/14/2003, Updated 03/25/13
I understand that CHT is in HIPAA compliance regarding maintaining the highest degree of confidentiality of my
personal and medical records information. A copy of the HIPAA Privacy Policy has been made available to me.
Assignment of Benefits and Payment Guarantee
I authorize insurance payment directly to CHT for services. This is a direct assignment of my rights and benefits under
this insurance policy. A photocopy of this assignment shall be considered as effective and valid as the original.
As the ultimate responsible party, I agree to pay CHT for the services provided to me. If any law (such as workers
compensation) or insurance contract prohibits payment for these services, I will cooperate and assist CHT in the provision
of information, authorizations, releases, or any other type of information necessary to allow for speedy collection from my
third-party payer. Where the law or an insurance contract does not prohibit payment by me, I acknowledge responsibility
for any and all account balances.
The Benefit Verification form is only an explanation of coverage obtained from my insurance company and is not a
guarantee of coverage. If the information provided by my insurance company is not accurate or the insurance company
changes its coverage, I will be responsible for payment for services.
I further understand that this agreement is binding regardless of any legal transaction currently in progress or initiated
during or after the course of my treatment unless agreed to in writing by myself and a CHT representative.
If I am a Medicare patient, then I, the above named patient and Medicare beneficiary, with Medicare number
and Medigap or supplement insurance policy number
, request that
payment of authorized Medicare and Medigap or supplemental benefits be made either to me or on my behalf to CHT for
any services furnished me by CHT. This authorization applies to all occasions of services until it is revoked.
Effective October 12, 2009
If you are unable to keep a scheduled appointment,
please call CHT 24 hours prior to your scheduled appointment time. Otherwise, there
will be a $35.00 charge for missed appointments or late cancellations.
All patients:
Patient/Guardian Signature
Date

Page 3 of 6
6/29/2023
COVENANT HAND THERAPY, PC PATIENT REGISTRATION
Please complete entire page. Patient Information and Brief Medical History
Last Name
First Name Middle Initial
Address
City
State
Zip Code
Home Phone
Cell Phone
Work Phone
Date of Birth
Gender: □ Male □ Female e-mail
Social Security Number N/A
Marital Status: □ Single □ Married □ Widow(er)
Were you referred to us because of an Accident? □ Auto □ Work □ Other incident □ No
Injury Date and Details
Patient’s Employer Name & Address
In case of Emergency, contact phone number
Do you now have -- or have you ever had -- any of the following?
Yes
No
Condition
Yes
No
Condition
Yes
No
Condition
Diabetes
Open Wounds related to
current condition
Thyroid Problems
Arthritis
Current Infection(s)
CVA /
Stroke
High Blood Pressure
Hypersensitivity to
Heat or Cold
Previous Fracture
Heart Disease
Allergies /
Asthma
Osteoporosis
Heart Attack
Hernia
Depression
Pacemaker or
Surgical Implant
Presently Pregnant
Anxiety
Vascular Disease
Seizures
Substance Abuse
Headaches /
Migraines
Metal in Body
Previous surgeries
Kidney Problems
Cancer /
Tumor
Other
If you answered “yes” on any of the above, please explain and give approximate date(s). Attached additional sheet if necessary.
Have you received any Occupational, Physical, or Speech Therapies,
or Chiropractic treatment during this current insurance plan year? □ No □ Yes - how much?
Are you NOW or WITHIN the LAST 60 DAYS receiving home-health care for any reason
OR any care at an out-Patient hospital or skilled nursing facility? No Yes
If YES, please give name and address of other provider:
Are you presently taking any medications? □ No □ Yes. If yes, please list:
The information above is correct to the best of my
knowledge.
Patient/Guardian Signature
Date
_
Page 4 of 6
6/29/2023
COVENANT HAND THERAPY, PC
1101 Ohio Drive, Suite 105, Plano, TX 75093 - phone 972-599-9594 - fax 972-599-9364
PAIN INFORMATION INTAKE
Pain Level Please mark your pain level on the scale below.
_____________________________________________________________
0 1 2 3 4 5 6 7 8 9 10
(none) (excruciating)
If none, stop here.
Pain Description Please mark all that apply in describing your pain.
Aching
Tender
Sharp
Dull
Burning
Throbbing
Numb
Tingling
Pins & Needles
Heavy
Tired
Tight
Shooting
Radiating
Cramping
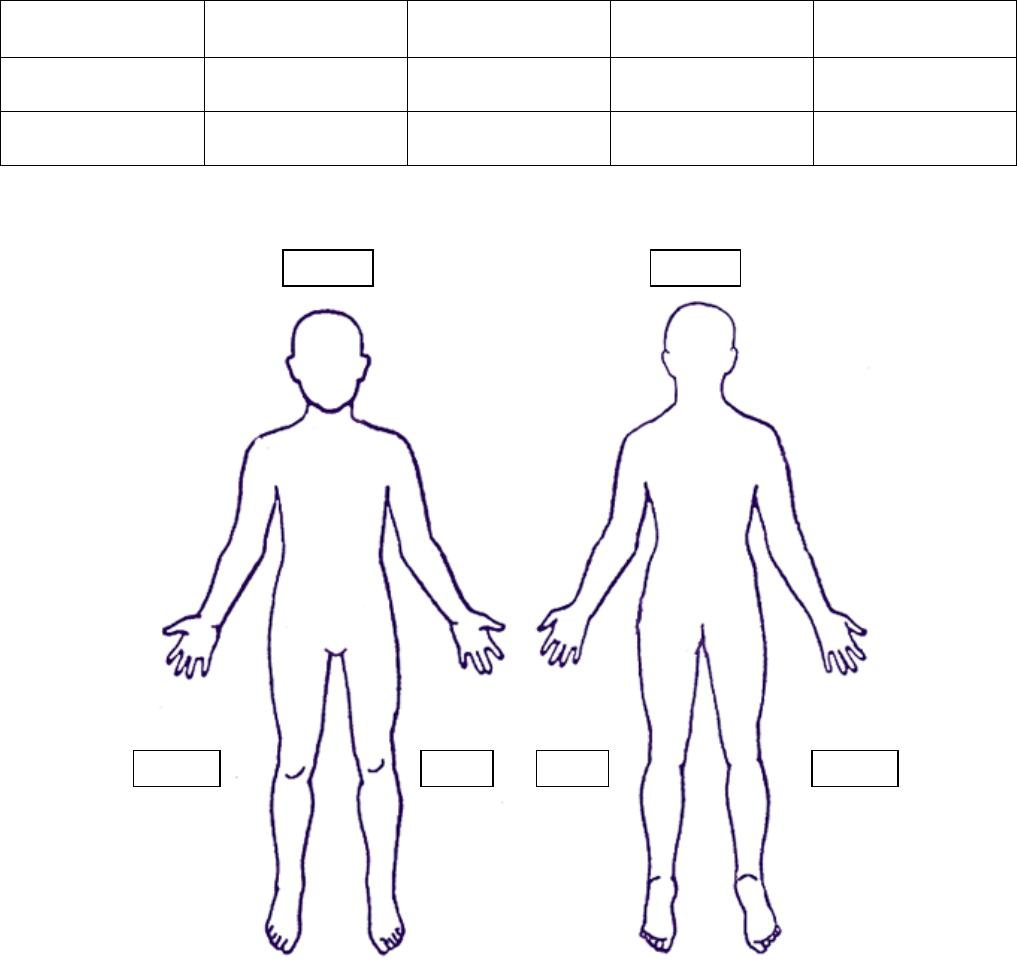
Pain Location Please mark where you feel the pain.
Patient’s Name ___________________________________ Date _________________
Front
Back
Right
RIght
Left
Left

Page 5 of 6
6/29/2023
COVENANT HAND THERAPY, PC
1101 Ohio Drive, Suite 105, Plano, TX 75093 - phone 972-599-9594 - fax 972-599-9364
Patient Authorization for Release of Information
Authorization is required for the Use or Disclosure of Information
Related to Treatment, Payment, Healthcare Operations unless otherwise permitted by Law or Rules
Patient’s Printed Name:
Patient’s Date of Birth: / /
Social Security Number: / /
I understand that my provider will need to communicate with my physician about my healthcare. I also understand
that in order for my insurance company to process and pay on claims for my treatment, they will also need information
about my healthcare; and by denying the insurance company such information, I will need to pay in full in cash for my
treatment at this facility.
CHT may release my information to:
My Doctor:
My Insurance Company:
Other:
Other:
Yes, you may release this information as long as my file is active
unless I herein specify a duration or expiration date.
If No, please specify duration or expiration date:
CHT may obtain my information:
I hereby authorize Covenant Hand Therapy, P.C. to obtain all medical records and/or professional information
FROM my physician or other medical professional AS IT RELATES TO MY CURRENT TREATMENT.
I may request restrictions as to how my health information may be used although CHT is not required to agree to
those restrictions if in violation of HIPAA compliance.
I may revoke this authorization in writing at any time, although CHT can proceed with uses and disclosures that
pertain to treatment, payment, or healthcare issues that take place before the consent was revoked.
I indicate understanding and consent for use of health information related to our service.
or
Signature of Patient Date Signature of Parent/Guardian Date
or Authorized Representative

Page 6 of 6
6/29/2023
FINANCIAL POLICY / BASIC INSURANCE INFORMATION
Covenant Hand Therapy,
P.C.
1101 Ohio Dr., Suite 105, Plano, TX
75093
972-599-9594 FAX 972-599-9364
We think that everyone benefits when there is a definite and clear understanding of our financial
policy prior to treatment.
1. ALL NEW patients are expected to present current and active proof of insurance. CHT
will bill your insurance company; however, you are responsible for your deductible,
co-pays and any amount that may not be covered by your insurance.
2. Deductible and co-pays are to be paid at time of service. This can be paid by cash,
check or credit card [American Express, Discover, MasterCard, Visa].
3. NSF CHECKS will be charged $30.00 plus the amount of the check. This is due upon
your next appointment or immediately upon notification.
4. MISSED/BROKEN APPOINTMENT CHARGE for any patient who cancels with less
than 24-hour notice or who does not present at the appointment time:
Therapy visit: $35.00
Orthotic (Splints) visit: $45.00
The fee is due upon the next visit. Patient must notify the clinic by phone (clinic voice mail is
available 24/7) of cancellation. 972-599-9594 Please do not email or text the clinic or
therapist.
IT IS YOUR RESPONSIBILITY TO MONITOR YOUR BENEFITS AND ANNUAL
MAXIMUM. We will be happy to assist you, but it is your responsibility.
PATIENTS WITH HMO PLANS: It is your responsibility to know and understand your HMO
plan. Generally, these plans require a patient co-pay at the time of service.
FOR YOUR CONVENIENCE WE ACCEPT CASH, PERSONAL CHECKS, AMERICAN
EXPRESS, DISCOVER, MASTERCARD, AND VISA, AS WELL AS CARE CREDIT.
We ask that you provide us with a valid credit card number to transfer any unpaid balance that is
delinquent over 90 days.
I HAVE READ AND AGREE TO THESE TERMS.
Patient/Guardian Signature Date
Patient PRINTED Name
[Policy effective 06/20/2012]
