
Mississippi Morbidity Report
Annual Summary
Selected Reportable Diseases
Mississippi – 2010
Volume 27, Number 12 December 2011
MISSISSIPPI STATE DEPARTMENT OF HEALTH
Mississippi Morbidity Report
Annual Summary
Selected Reportable Diseases
Mississippi – 2010
Page Left Blank Intentionally
Table of Contents
Preface .................................................................................................................................. 5
Mississippi Public Health Districts & Health Officers ........................................................... 6
Reportable Disease List ........................................................................................................ 7
Arboviral Infections (mosquito-borne) ............................................................................. 10
Eastern Equine Encephalitis (EEE) .......................................................................... 11
LaCrosse Encephalitis ............................................................................................. 12
St. Louis Encephalitis ............................................................................................... 13
West Nile Virus ......................................................................................................... 14
Campylobacteriosis ........................................................................................................... 17
Chlamydia .......................................................................................................................... 20
Cryptosporidiosis ................................................................................................................ 23
E. coli O157:H7/ HUS ........................................................................................................... 26
Gonorrhea .......................................................................................................................... 29
Haemophilus influenzae type b (Hib), invasive ............................................................... 32
Hepatitis A ........................................................................................................................... 34
Hepatitis B, acute ............................................................................................................... 36
HIV Disease ......................................................................................................................... 39
Influenza.............................................................................................................................. 43
Legionellosis ....................................................................................................................... 47
Listeriosis ............................................................................................................................. 48
Lyme Disease ..................................................................................................................... 50
Measles ............................................................................................................................... 51
Meningococcal disease, invasive .................................................................................... 53
Mumps ................................................................................................................................ 56
Pertussis ............................................................................................................................... 57
Pneumococcal disease, invasive ..................................................................................... 60
Rabies .................................................................................................................................. 62
Rocky Mountain spotted fever .......................................................................................... 65
Rubella ................................................................................................................................ 67
Salmonellosis ...................................................................................................................... 68
Shigellosis ............................................................................................................................ 71
Syphilis ................................................................................................................................ 74
Tuberculosis ........................................................................................................................ 80
Varicella .............................................................................................................................. 85
Vibrio disease ..................................................................................................................... 86
Events of Public Health Significance ................................................................................. 89
Botulism Case ...................................................................................................... 89
Brucellosis Cases ................................................................................................. 90
Legionella Outbreak ........................................................................................... 91
Norovirus Outbreak ............................................................................................. 92
Salmonella Outbreak .......................................................................................... 93
Varicella Outbreak #1 ........................................................................................ 93
Varicella Outbreak #2 ........................................................................................ 93
Reportable Disease Statistics ............................................................................................ 94
List of Contacts, Editors and Contributors ......................................................................... 96
General References ........................................................................................................... 97

5
Preface
Public health surveillance involves the systematic collection, analysis and dissemination
of data regarding adverse health conditions. The data are used to monitor trends and
identify outbreaks in order to assess risk factors, target disease control activities,
establish resource allocation priorities and provide feedback to the medical community
and the public. These data support public health interventions for both naturally
occurring and intentional spread of disease.
Statistics incorporated into tables, graphs and maps reflect data reported from health
care providers who care for Mississippi residents. Cases counted have met the
surveillance case definitions of the CDC and the Council of State and Territorial
Epidemiologists (CSTE). Unless otherwise noted all rates are per 100,000 population.
Data are based on “event” date of the case with the exception of TB in which the case
confirmation date is used. The “event” date is defined as the earliest known date
concerning a case and is hierarchical (onset, diagnosis, laboratory date or date of
report to the health department).
Mississippi law (Section 41-3-17, Mississippi Code of 1972 as amended) authorizes the
Mississippi State Board of Health, under which the Mississippi State Department of Health
(MSDH) operates, to establish a list of diseases which are reportable. The reportable
disease list and the Rules and Regulations Governing Reportable Diseases and
Conditions may be found online at
http://www.msdh.state.ms.us/msdhsite/_static/14,0,194.html. Class 1 diseases,
reportable by telephone at first knowledge or suspicion, are those to which the MSDH
responds immediately to an individual case; Class 2 diseases, those reportable within a
week of diagnosis, and Class 3 diseases, reportable only by laboratories; do not
necessitate an immediate response to an individual case.
To report a case of any reportable disease or any outbreak, please call 601-576-7725
during working hours in the Jackson area, or 1-800-556-0003 outside the Jackson area.
For reporting tuberculosis, you also may call 601-576-7700, and for reporting STD’s or
HIV/AIDS, you may call 601-576-7723. For emergency consultation or reporting Class 1
diseases or outbreaks nights and weekends please call 601-576-7400.
The data included in the following document have come from physicians, nurses,
clinical laboratory directors, office workers and other health care providers across the
state who called or sent in reports. Without these individuals, public health surveillance
and response would be incapacitated. For your dedication to this important part of
public health information, we thank you.
Mary Currier, MD, MPH
State Health Officer

6
Mississippi Public Health Districts & Health Officers
Public Health
Districts
Northwest Public Health
District I
Dr. Alfio Rausa
662.563.5603
Northeast Public Health
District II
Dr. Jessie Taylor
662.841.9015
Delta/Hills Public Health
District III
Dr. Alfio Rausa
662.453.4563
Tombigbee Public Health
District IV
Dr. Robert Curry
662.323.7313
West Central Public Health
District V
Dr. Rebecca James
601.978.7864
East Central Public Health
District VI
Dr. Rebecca James
601.482.3171
Southwest Public Health
District VII
Dr. Thomas Dobbs
601.684.9411
Southeast Public Health
District VIII
Dr. Thomas Dobbs
601.544.6766
Coastal Plains Public Health
District IX
Dr. Robert Travnicek
228.436.6770

7
Reportable Disease List
Mississippi State Department of Health
List of Reportable Diseases and Conditions
Reporting Hotline: 1-800-556-0003
Monday - Friday, 8:00 am - 5:00 pm
To report inside Jackson telephone area or for consultative services
Monday - Friday, 8:00 am - 5:00 pm: (601) 576-7725
Phone
Fax
Epidemiology
(601) 576-7725
(601) 576-7497
STD/HIV
(601) 576-7723
(601) 576-7909
TB
(601) 576-7700
(601) 576-7520
Class 1 Conditions may be reported nights, weekends and holidays by calling: (601) 576-7400
Class 1: Diseases of major public health importance which shall be reported directly to the
Mississippi State Department of Health (MSDH) by telephone within 24 hours of first
knowledge or suspicion. Class 1 diseases and conditions are dictated by requiring an
immediate public health response. Laboratory directors have an obligation to report
laboratory findings for selected diseases (refer to Appendix B of the Rules and
Regulations Governing Reportable Diseases and Conditions).
Any Suspected Outbreak (including foodborne and waterborne outbreaks)
(Possible biological weapon agents appear in bold italics)
Anthrax
Encephalitis (human)
Smallpox
Arboviral infections including but
Glanders
Staphylococcus aureus,
not limited to those due to:
Haemophilus influenzae Invasive
vancomycin resistant
California encephalitis virus
Disease
†‡
(VRSA) or vancomycin
Eastern equine encephalitis
Hemolytic uremic syndrome (HUS),
intermediate (VISA)
virus
post- diarrheal
Syphilis (including
LaCrosse virus
Hepatitis A
congenital)
Western equine encephalitis
HIV infection, including AIDS
Tuberculosis
virus
Influenza-associated pediatric
Tularemia
St. Louis encephalitis virus
mortality (<18 years of age)
Typhoid fever
West Nile virus
Measles
Typhus fever
Botulism (including foodborne,
Melioidosis
Varicella infection,
infant or wound)
Neisseria meningitidis Invasive
primary, in patients >15
Brucellosis
Disease
†‡
years of age
Chancroid
Pertussis
Viral hemorrhagic fevers
Cholera
Plague
(filoviruses [e.g. Ebola,
Creutzfeldt-Jakob disease,
Poliomyelitis
Marburg] and,
including new variant
Psittacosis
Arenaviruses [e.g.,Lassa,
Diphtheria
Q fever
Machupo])
Escherichia coli O157:H7 and any
Rabies (human or animal)
Yellow fever
shiga toxin-producing E. coli
Ricin intoxication (castor
(STEC)
beans)
Any unusual disease or manifestation of illness, including but not limited to the appearance of a novel
or previously controlled or eradicated infectious agent, or biological or chemical toxin.

8
Class 2: Diseases or conditions of public health importance of which individual cases shall be
reported by mail, telephone, fax or electronically, within 1 week of diagnosis. In
outbreaks or other unusual circumstances they shall be reported the same as Class 1.
Class 2 diseases and conditions are those for which an immediate public health
response is not needed for individual cases.
Chlamydia trachomatis, genital
Lyme disease
Rubella (including
infection
Malaria
congenital)
Dengue
Meningitis other than
Salmonellosis
Ehrlichiosis
meningococcal or H. influenzae
Shigellosis
Enterococcus, invasive infection
‡
,
Mumps
Spinal cord injuries
vancomycin resistant
M. tuberculosis infection (positive
Streptococcus
Gonorrhea
TST or positive IGRA***) in children
pneumoniae, invasive
Hepatitis (acute, viral only) Note -
< 15 years of age
infection
‡
Hepatitis A requires Class 1
Noncholera vibrio disease
Tetanus
Legionellosis
Poisonings* (including elevated
Trichinosis
Listeriosis
blood lead levels**)
Viral encephalitis in horses
Rocky Mountain spotted fever
and ratites
†
Usually presents as meningitis or septicemia, or less commonly as cellulitis, epiglottitis, osteomyelitis,
pericarditis or septic arthritis.
‡
Specimen obtained from a normally sterile site.
*Reports for poisonings shall be made to Mississippi Poison Control Center, UMMC 1-800-222-1222.
**Elevated blood lead levels (as designated below) should be reported to the MSDH Lead Program at
(601) 576-7447.
Blood lead levels (venous) of >10 µg/dL in children less than 16 years of age
Blood lead levels (venous) of >25 µg/dL in those 16 years or older
***TST- tuberculin skin test; IGRA- Interferon-Gamma Release Assay
Except for rabies, equine, and ratite encephalitis, diseases occurring in animals are not required to be
reported to the MSDH.

9
Class 3: Laboratory based surveillance. To be reported by laboratories only. Diseases or
conditions of public health importance of which individual laboratory findings shall be
reported by mail, telephone, fax or electronically within one week of completion of
laboratory tests (refer to Appendix B of the Rules and Regulations Governing Reportable
Diseases and Conditions).
All blood lead test results
Chagas Disease (American
Hepatitis C infection
Blastomycosis
Trypanosomiasis)
Histoplasmosis
Campylobacteriosis
Cryptosporidiosis
Nontuberculous
Hansen disease (Leprosy)
mycobacterial disease
Class 4: Diseases of public health importance for which immediate reporting is not necessary for
surveillance or control efforts. Diseases and conditions in this category shall be reported
to the Mississippi Cancer Registry within six months of the date of first contact for the
reportable condition.
The National Program of Cancer Registries at the Centers for Disease Control and Prevention
requires the collection of certain diseases and conditions. A comprehensive reportable list
including ICD9CM codes is available on the Mississippi Cancer Registry website,
http://mcr.umc.edu/documents/ReportableCases10-09andlater.pdf.
Each record shall provide a minimum set of data items which meets the uniform standards
required by the National Program of Cancer Registries and documented in the North American
Association of Central Cancer Registries (NAACCR).

10
Arboviral Infections (mosquito-borne)
Background
Arthropod-borne viral (arboviral) diseases in Mississippi are limited to a few types
transmitted by mosquitoes. In this state, there are four main types of arboviral infections
that have been reported: West Nile virus (WNV), St. Louis encephalitis (SLE), eastern
equine encephalitis (EEE), and LaCrosse encephalitis (LAC). WNV and SLE are members
of the Flavivirus genus, while EEE is an Alphavirus, and LAC is in the California virus group
of Bunyaviruses.
Infections do not always result in clinical disease. When illness occurs, symptoms can
range from a mild febrile illness to more severe cases of neuroinvasive disease with
symptoms of encephalitis and/or meningitis. Neuroinvasive disease can result in long
term residual neurological deficits or death. The proportion of infected persons who
develop symptoms depends largely on the age of the persons and the particular virus
involved.
Mosquito borne arboviral infections are typically more common in the warmer months
when mosquitoes are most active, but WNV cases have been reported year round. All
are transmitted by the bite of an infected mosquito, but the mosquito vectors and their
habitats differ. Infections are not transmitted by contact with an infected animal or
other person; humans and horses are “dead end” or incidental hosts. Rare instances of
WNV transmission have occurred transplacentally and through transplanted organs
and blood transfusions.
Methods of Control
The methods of controlling mosquito-borne infections are essentially the same for all the
individual diseases. The best preventive strategy is to avoid contact with mosquitoes.
Reduce time spent outdoors, particularly in early morning and early evening hours
when mosquitoes are most active; wear light-colored long pants and long-sleeved
shirts; and apply mosquito repellant to exposed skin areas. Reduce mosquito breeding
areas around the home and workplace by eliminating standing or stagnant water.
Larvacides are effective when water cannot easily be drained.
Mosquito Surveillance
Mosquitoes are collected throughout the state for West Nile and other arboviral testing
to provide information regarding the burden and geographic distribution of infected
vectors. Mosquitoes are collected by local mosquito programs and MSDH personnel
and submitted as pools of 5-50 mosquitoes for testing. In 2010, 439 mosquito pools were
submitted to the MSDH Public Health Laboratory (PHL) for WNV, SLE, and EEE testing.

11
Arboviral Testing
The MSDH PHL performs an arboviral panel consisting of IgM testing for WNV and SLE,
and, for patients less than 25 years of age, LAC IgM. Clinicians are encouraged to call
MSDH Epidemiology or the PHL for specifics and indications for arboviral testing. 732
samples were submitted to the MSDH PHL for arboviral testing in 2010.
Please refer to the individual disease summaries for information on and epidemiology of
each specific arbovirus.
Eastern Equine Encephalitis (EEE)
2010 Case Total
0
2010 rate/100,000
0.0
2009 Case Total
0
2009 rate/100,000
0.0
Clinical Features
Clinical illness is associated with symptoms that can range from a mild flu-like illness
(fever, headache, muscle aches) to seizures and encephalitis progressing to coma and
death. The case fatality rate is 30-50%. Fifty percent of those persons who recover from
severe illness will have permanent mild to severe neurological damage. Disease is more
common in young children and in persons over the age of 55.
Infectious Agent
Eastern equine encephalitis virus, a member of the genus Alphavirus.
Reservoir
Maintained in a bird-mosquito cycle. Humans and horses are incidental hosts.
Transmission
Through the bite of an infected mosquito, usually Coquilletidia perturbans. This
mosquito, known as the salt and pepper or freshwater marsh mosquito, breeds mainly in
marshy areas.
Incubation
3-10 days (generally within 7 days).
Reporting Classification
Class 1.

12
Epidemiology and Trends
Human cases are relatively infrequent largely because primary transmission takes place
in and around marshy areas where human populations are generally limited. There
were no reported cases of EEE in Mississippi in 2010. The last two reported cases of EEE
occurred in October 2002.
Horses also become ill with EEE and are dead end hosts. Infected horses can serve as
sentinels for the presence of EEE, and can indicate an increased risk to humans. The
Mississippi Board of Animal Health reports equine infections to MSDH, and in 2010, 19
horses tested positive for EEE. The EEE-positive horses were located in the southern part
of the state with 89% of the horses reported from District IX and District VIII. Reports were
also received from Pike (1) and Scott (1) counties. There were no reported EEE positive
mosquito pools in 2010.
LaCrosse Encephalitis
2010 Case Total
0
2010 rate/100,000
0.0
2009 Case Total
0
2009 rate/100,000
0.0
Clinical Features
Clinical illness occurs in about 15% of infections. Initial symptoms of LaCrosse
encephalitis infection include fever, headache, nausea, vomiting and lethargy. More
severe symptoms usually occur in children under 16 and include seizures, coma, and
paralysis. The case fatality rate for clinical cases of LaCrosse encephalitis is about 1%.
Infectious Agent
LaCrosse encephalitis virus, in the California serogroup of Bunyaviruses.
Reservoir
Chipmunks and squirrels.
Transmission
Through the bite of an infected Ochlerotatus triseriatus mosquito (commonly known as
the tree-hole mosquito). This mosquito is commonly associated with tree holes and
most transmission tends to occur in rural wooded areas. However, this species will also
breed in standing water in containers or tires around the home.
Incubation
7-14 days.

13
Reporting Classification
Class 1.
Epidemiology and Trends
Reported LaCrosse encephalitis remains relatively rare in Mississippi, with 15 reported
cases since 1999. There were no reported cases of LaCrosse encephalitis in 2010.
Of the 15 total cases since 1999, 53% were in females. The ages ranged from 3 months
to 78 years of age, with 93% of the cases being under the age of 15.
Another Bunyavirus in the California group, Jamestown Canyon encephalitis virus, has
also been seen in Mississippi, with one reported case in 1993, one in 2006, and one in
2008. There were no reported cases of Jamestown Canyon encephalitis virus in 2010.
St. Louis Encephalitis
2010 Case Total
0
2010 rate/100,000
0.0
2009 Case Total
2
2009 rate/100,000
0.1
Clinical Features
Less than 1% of infections result in clinical illness. Individuals with mild illness often have
only a headache and fever. The more severe illness, meningoencephalitis, is marked
by headache, high fever, neck stiffness, stupor, disorientation, coma, tremors,
occasional convulsions (especially in infants) and spastic (but rarely flaccid) paralysis.
The mortality rate from St. Louis encephalitis (SLE) ranges from 5 to 30%, with higher rates
among the elderly.
Infectious Agent
St. Louis encephalitis virus, a member of the genus Flavivirus.
Reservoir
Maintained in a bird-mosquito cycle. Infection does not cause a high mortality in birds.
Transmission
Through the bite of an infected mosquito generally belonging to genus Culex (Culex
quinquefasciatus, Culex pipiens), the southern house mosquito. This mosquito breeds in
standing water high in organic materials, such as containers and septic ditches near
homes.

14
Incubation
5-15 days.
Reporting Classification
Class 1.
Epidemiology and Trends
The number of reported SLE cases fluctuates annually. There were no cases reported in
2004, 2006, 2008 or 2010, but there were nine cases with one death reported in 2005,
two reported cases in both 2007 and 2009. There were no deaths due to SLE in 2007 or
2009.
Mississippi had no reported cases of SLE in 2010. No positive SLE mosquito pools were
reported in 2010.
West Nile Virus
2010 Case Total
8
2010 rate/100,000
0.3
2009 Case Total
53
2009 rate/100,000
1.8
Clinical Features
Clinical illness occurs in approximately 20% of infected individuals. Most with clinical
manifestations will develop the milder West Nile fever, which includes fever, headache,
fatigue, and sometimes a transient rash. About 1 in 150 infected persons develop more
severe West Nile neuroinvasive disease ranging from symptoms compatible with
meningitis to encephalitis. Encephalitis is the most common form of severe illness and is
usually associated with altered consciousness that may progress to coma. Focal
neurological deficits and movement disorders may also occur. West Nile poliomyelitis, a
flaccid paralysis syndrome, is seen less frequently. The elderly and
immunocompromised are at highest risk of severe disease.
Infectious Agent
West Nile virus, a member of the genus Flavivirus.
Reservoir
WNV is maintained in a bird mosquito cycle, has been detected in more than 317
species of birds, particularly crows and jays.

15
Transmission
Primarily through the bite of an infected southern house mosquito (Culex
quinquefasciatus). This mosquito breeds in standing water with heavy organic matter.
Incubation
3-15 days.
Reporting Classification
Class 1.
Epidemiology and Trends
In Mississippi, West Nile virus was first isolated in horses in 2001 followed by human
infections in 2002 with 192 cases reported. The years following saw a decrease in the
number of reported infections; however in 2006, there was a resurgence of 184 cases
(Figure 1). In 2010, there were 8 reported cases with no deaths.
Figure 1
*U.S. data: 66 cases in 2001.
WNV is now thought to be endemic in Mississippi, and the mosquito vector is present the
entire year. Human illness can occur year round, but is most prevalent from July to
October. August and September are usually the peak months (Figure 2).

16
Figure 2
Of the 8 WNV cases reported in 2010, 5 (63%) were classified as WNV fever and 3 (38%)
were encephalitis. The cases ranged in age from 7 to 77 years, with a median age of
51 years (Figure 3).
Figure 3
WNV infection can occur in any part of the state, and since 2001, activity (human
cases, positive mosquito pools, horses or birds) has been reported in every Mississippi

17
County except Issaquena. The cases in 2010 were reported from the following counties:
Calhoun (1), Coahoma (1), Leflore (3), Scott (1), Tallahatchie (1), and Tate (1).
A total of five mosquito pools tested positive for WNV in 2010. Horses may also become
ill with WNV and can act as sentinels for the presence of infected mosquitoes. The
Mississippi Board of Animal Health reports equine infections to MSDH. In 2010, two horses
tested positive for WNV with one each being from Tippah and Forrest counties.
Campylobacteriosis
2010 Case Total
128
2010 rate/100,000
4.3
2009 Case Total
110
2009 rate/100,000
3.7
Clinical Features
Campylobacteriosis is a zoonotic bacterial disease of variable severity ranging from
asymptomatic infections to clinical illness presenting with diarrhea, abdominal pain,
fever, and nausea and vomiting. Symptoms typically resolve after one week, but may
persist for weeks if untreated. Rare post-infectious syndromes include reactive arthritis
and Guillain-Barré syndrome (GBS).
Infectious Agent
Campylobacter jejuni (C. jejuni) causes most cases of diarrheal illness in humans.
Reservoir
Commonly present in cattle and poultry.
Transmission
Transmission mainly occurs through ingestion of undercooked meat, usually poultry, but
occasionally contaminated food or water or raw milk. The number of organisms
required to cause infection is low.
Incubation
Average incubation is 2-5 days, with a range from 1-10 days.
Period of Communicability
Person to person transmission does not typically occur, though the infected individual
may shed organisms for up to 7 weeks without treatment.

18
Methods of Control
Disease prevention includes promotion of proper food handling, good hand washing,
particularly after handling raw meats, and after contact with feces of dogs and cats.
Pasteurizing milk and chlorinating water are also important. Symptomatic individuals
should be excluded from food handling or care of patients in hospitals or long term
care facilities.
Reporting Classification
Class 3.
Epidemiology and Trends
In 2010, there were 128 reported cases of campylobacteriosis in Mississippi; this was
slightly increased from the 110 cases reported in 2009 and the three-year (2007-2009)
average of 118 cases (Figure 4).
Figure 4
Campylobacter infections are typically more common in the warmer months, as are
many enteric illnesses, with 41% of the total 2010 cases occurring in June, July, and
August; however cases are reported to MSDH year round (Figure 5). The highest rates of
infection are in children less than five years of age. In 2010, 28% of all reported cases
were in children younger than five years of age (Figure 6).

19
Figure 5
Figure 6

20
Chlamydia
2010 Case Total
21,422
2010 rate/100,000
721.9
2009 Case Total
23,592
2009 rate/100,000
799.2
Clinical Features
A sexually transmitted bacterial infection causing urethritis in males and cervicitis in
females. Urethritis in men presents with scant to moderate mucopurulent urethral
discharge, urethral itching, and dysuria. Cervicitis presents as a mucopurulent
endocervical discharge, often with endocervical bleeding. The most significant
complications in women are pelvic inflammatory disease and chronic infections, both
of which increase the risk of ectopic pregnancy and infertility. Perinatal transmission of
chlamydia occurs when an infant is exposed to the infected cervix during birth resulting
in chlamydial pneumonia or conjunctivitis. Asymptomatic infection may be found in 1%-
25% of sexually active men. Up to 70% of sexually active women with chlamydial
infections may also be asymptomatic.
Infectious Agent
Chlamydia trachomatis, an obligate intracellular bacteria. Immunotypes D through K
have been identified in 35-50% of nongonococcal urethritis.
Reservoir
Humans.
Transmission
Transmitted primarily through sexual contact.
Incubation
Incubation period is poorly defined, ranging from 7 to 14 days or longer.
Period of Communicability
Unknown.
Methods of Control
Prevention and control of chlamydia are based on behavior change, effective
treatment, and mechanical barriers. Condoms and diaphragms provide some degree
of protection from transmission or acquisition of chlamydia. Effective treatment of the
infected patient and their partners, from 60 days prior to the onset of symptoms, is
recommended.

21
Reporting Classification
Class 2.
Epidemiology and Trends
Chlamydia is the most frequently reported bacterial sexually transmitted disease in the
United States and in Mississippi. In 2010, 21,422 cases of chlamydia were reported in
Mississippi, a 13% increase from 2006 (19,001). Mississippi has reported case rates higher
than the United States average (Figure 7) for several years, and when compared to
other states, Mississippi has the country’s highest rate. The overall increase in cases can
be partially attributed to aggressive statewide screening for chlamydia in all MSDH STD,
family planning, and prenatal clinics beginning April 2004.
Figure 7
Chlamydia was reported in every public health district, with the highest incidence
noted in Public Health District III (Figure 8).
Implementation
of statewide
screening

22
Figure 8
Chlamydia Incidence by Public Health District, Mississippi, 2010
District
Cases
Rate*
I
2459
768.5
II
1732
480.1
III
2744
1266.2
IV
1707
691.2
V
5300
838.8
VI
2029
830.0
VII
1397
799.2
VIII
1993
653.7
IX
2061
441.4
State
21,422
721.9
*per 100,000 population
Chlamydia infections were reported over a range of age groups, but the largest
proportion was reported among 15-24 year olds, accounting for 76% of the reported
cases (Figure 9). African Americans accounted for 83% of the reported cases in which
race was known (Figure 10). In 2010, the rate of chlamydia infections for African
Americans (1278.2 per 100,000) was nearly nine times the rate for whites (143.6 per
100,000).
Figure 9

23
Figure 10
Cryptosporidiosis
2010 Case Total
24
2010 rate/100,000
0.8
2009 Case Total
19
2009 rate/100,000
0.6
Clinical Features
A parasitic infection characterized by profuse, watery diarrhea associated with
abdominal pain. Symptoms include anorexia, weight loss, fever, and nausea and
vomiting less frequently. Symptoms often wax and wane and but generally disappear
in 30 days or less in healthy people. Asymptomatic infections do occur. The disease
may be prolonged and fulminant in immunodeficient individuals unable to clear the
parasite. Children under 2, animal handlers, travelers, men who have sex with men,
and close personal contacts of infected individuals are more prone to infection.
Infectious Agent
Cryptosporidium parvum, a coccidian protozoan, is associated with human infection.
Reservoir
Humans, cattle and other domesticated animals.
Transmission
Fecal-oral, which includes person-to-person, animal-to-person, waterborne (including
recreational use of water) and foodborne transmission. Oocysts are highly resistant to

24
chemicals used to purify drinking water and recreational water (swimming pools, water
parks). The infectious dose can be as low as 10 organisms.
Incubation
1 to 12 days (average 7 days).
Period of Communicability
As long as oocysts are present in the stool. Oocysts may be shed in the stool from the
onset of symptoms to several weeks after symptoms resolve.
Methods of Control
Education of the public regarding appropriate personal hygiene, including
handwashing. Symptomatic individuals with a diagnosis of cryptosporidiosis should not
use public recreational water (e.g., swimming pools, lakes, ponds) while they have
diarrhea and for at least 2 weeks after symptoms resolve. It is recommended that
infected individuals be restricted from handling food, and symptomatic children be
restricted from attending daycare until free of diarrhea. Prompt investigation of
common food or waterborne outbreaks is important for disease control and prevention.
Reporting Classification
Class 3.
Epidemiology and Trends
There were 24 reported cases of cryptosporidiosis in 2010, which is comparable to 2009
with 19 reported cases. In a typical year, usually 3-29 cases are reported (Figure 11).
The reported cases ranged in age from 3 months to 83 years (Figure 12).

25
Figure 11
Figure 12

26
E. coli O157:H7/ HUS
2010 Case Total
24
2010 rate/100,000
0.8
2009 Case Total
6
2009 rate/100,000
0.2
Clinical Features
Escherichia coli (E. coli) O157:H7 is the most virulent serotype of the Shiga toxin-
producing E. coli (STEC), and is associated with diarrhea, hemorrhagic colitis, hemolytic-
uremic syndrome (HUS), and postdiarrheal thrombotic thrombocytopenic purpura (TTP).
Symptoms often begin as nonbloody diarrhea but can progress to diarrhea with occult
or visible blood. Severe abdominal pain is typical, and fever is usually absent. The very
young and the elderly are more likely to develop severe illness and HUS, defined as
microangiopathic hemolytic anemia, thrombocytopenia, and acute renal dysfunction.
HUS is a complication in about 8% of E. coli O157:H7 infections. Supportive care is
recommended as antibiotic use may increase the risk of progression to HUS.
Infectious Agent
E. coli are gram negative bacilli. E. coli O157:H7 is thought to cause more than 90% of
all diarrhea-associated HUS.
Reservoir
Cattle, to a lesser extent other animals, including sheep, deer, and other ruminants.
Humans may also serve as a reservoir for person-to-person transmission.
Transmission
Mainly through ingestion of food contaminated with ruminant feces, usually
inadequately cooked hamburgers; also contaminated produce or unpasteurized milk.
Direct person-to-person transmission can occur in group settings. Waterborne
transmission occurs both from contaminated drinking water and from recreational
waters.
Incubation
2-10 days, with a median of 3-4 days.
Period of Communicability
Duration of excretion is typically 1 week or less in adults but can be up to 3 weeks in
one-third of children. Prolonged carriage is uncommon.

27
Methods of Control
Education regarding proper food preparation and handling and good hand hygiene is
essential in prevention and control. Pasteurization of milk and juice is important.
MSDH investigates all reported cases of HUS and E. coli O157:H7 infections. All isolates
should be submitted to the Public Health Laboratory (PHL) for molecular subtyping, or
DNA “fingerprinting”, with pulsed-field gel electrophoresis (PFGE). Isolate information is
submitted to a national tracking system (PulseNet), a network of public health and food
regulatory agencies coordinated by the CDC. This system facilitates early detection of
common source outbreaks, even if the affected persons are geographically far apart,
and assists in rapidly identifying the source of outbreaks.
Reporting Classification
Class1.
Epidemiology and Trends
In 2010, twenty-four E. coli O157:H7 infections were reported to MSDH; seven of which
resulted in HUS. On average, six infections have been reported annually over the past
three years (2007-2009) (Figure 13). There were no deaths reported in Mississippi in 2010.
Of the 43 cases of E. coli O157:H7/HUS that were reported to MSDH between 2007 and
2010, 58% occurred in children less than 10 years of age (Figure 14).
Thirteen (54%) of these infections were linked to a familial cluster in Oktibbeha County
and ranged in age from 6 months to 57 years of age. Five of the cases required
hospitalization and 3 developed HUS. Inadequate wastewater disposal was noted in
propagating the spread of infection.
A separate cluster of three cases was associated with a daycare exposure in
Washington County. All three of the cases required hospitalization and two developed
HUS. No specific source of illness was identified.

28
Figure 13
* 2006 U.S. rate includes E. coli O157:H7; shiga toxin positive, serogroup non-O157; and shiga toxin positive, not serogrouped.
Figure 14

29
Gonorrhea
2010 Case Total
6,196
2010 rate/100,000
208.8
2009 Case Total
7,241
2009 rate/100,000
245.3
Clinical Features
A bacterial infection associated primarily with infection of the urogenital tract
producing symptoms of discharge and dysuria. Other less common sites of infection
include: pharynx, rectum, conjunctiva, and blood.
Complications associated with gonorrhea infection in men consist of epididymitis,
penile lymphangitis, penile edema, and urethral strictures. The primary complication
associated with gonorrhea infection in women is pelvic inflammatory disease, which
produces symptoms of lower abdominal pain, cervical discharge, and cervical motion
pain. Asymptomatic infections do occur. Pregnant women infected with gonorrhea
may transmit the infection to their infants during a vaginal delivery. Infected infants can
develop conjunctivitis leading to blindness if not rapidly and adequately treated.
Septicemia can also occur in infected infants.
Infectious Agent
Neisseria gonorrhoeae, an intracellular gram-negative diplococcus.
Reservoir
Humans.
Transmission
Gonorrhea is transmitted primarily by sexual contact, but transmission from the infected
cervix to an infant during birth occurs.
Incubation
In men, the incubation period is primarily 2-5 days, but may be 10 days or longer. In
women, it is more unpredictable, but most develop symptoms less than 10 days after
exposure.
Period of Communicability
In untreated individuals, communicability can last for months; but if an effective
treatment is provided communicability ends within hours.

30
Methods of Control
Prevention and control of gonorrhea are based on education, effective treatment, and
mechanical barriers. Condoms and diaphragms provide some degree of protection
from transmission or acquisition of gonorrhea. Effective treatment of the infected
patient and their partners from 60 days prior to the onset of symptoms is recommended.
Reporting Classification
Class 2.
Epidemiology and Trends
Gonorrhea is the second most commonly reported notifiable disease in the United
States. In Mississippi, from 2003-2007, the number of gonorrhea cases increased 31.4%,
from 6,328 to 8,315 cases (Figure 15). Although there was a slight decrease in cases
since 2007, Mississippi still has the highest case rate of gonorrhea in the United States.
Figure 15
Gonorrhea was reported in every public health district, with the highest incidence
noted in Public Health District III (Figure 16).

31
Figure 16
Gonorrhea Incidence by Public Health District, Mississippi, 2010
District
Cases
Rate*
I
606
189.4
II
438
121.4
III
867
400.1
IV
449
181.8
V
1805
285.7
VI
591
241.8
VII
328
187.6
VIII
552
181.0
IX
560
119.9
State
6,196
208.8
*per 100,000 population
Although the burden of disease impacted individuals in most of the age groups, 70% of
reported cases were among 15-24 year olds (Figure 17). African Americans accounted
for 90% of the reported cases in which race was known (Figure 18). In 2010, the rate of
gonorrhea infections for African Americans (420.7 per 100,000) was sixteen times the
rate of whites (26.1 per 100,000).
Figure 17

32
Figure 18
Haemophilus influenzae type b (Hib), invasive
2010 Case Total
0
2010 rate/100,000
0.0
2009 Case Total
0
2009 rate/100,000
0.0
Clinical Features
Haemophilus influenzae, type b (Hib) is an invasive bacterial disease, particularly
among infants, that can affect many organ systems. Invasive disease usually begins as
a bloodstream infection, with bacteria spreading to distant sites. Epiglottitis,
pneumonia, septic arthritis, and septicemia are other forms of invasive disease. Hib
meningitis presents with fever, decreased mental status and nuchal rigidity. Neurologic
sequelae can occur in 15-30% of survivors, with hearing impairment the most common.
Case fatality rate is 2-5% even with antimicrobial therapy. Peak incidence is usually in
infants 6-12 months of age; Hib disease rarely occurs beyond 5 years of age. In the
prevaccine era, meningitis accounted for 50-60% of all cases of invasive disease. Since
the late 1980’s, with the licensure of Hib conjugate vaccines, Hib meningitis has
essentially disappeared in the U.S.
Infectious Agent
Haemophilus influenzae type b, a gram-negative encapsulated bacterium.
Reservoir
Humans, asymptomatic carriers.

33
Transmission
Respiratory droplets and contact with nasopharyngeal secretions during the infectious
period.
Incubation
Uncertain; probably short, 2-4 days.
Period of Communicability
As long as organisms are present and up to 24-48 hours after starting antimicrobial
therapy.
Methods of Control
Two Hib conjugate vaccines are licensed for routine childhood vaccination. The
number of doses in the primary series is dependent on the type of vaccine used. A
primary series of PRP-OMP (PedvaxHIB®) vaccine is two total doses, at 2 and 4 months
of age; the primary series with PRP-T (ActHIB®) requires three total doses, given at 2, 4
and 6 months of age. A booster dose at 12-15 months of age is recommended
regardless of which vaccine is used for the primary series. Vaccination with Hib
containing vaccines may decrease the carriage rate, decreasing the chances of
infection in unvaccinated in children. Immunization is not recommended for children
over 5 years of age.
The Mississippi State Department of Health (MSDH) investigates all reported suspected
Hib cases and provides prophylactic antibiotics (rifampin) for all household contacts
with one or more children under one year old or in households with children 1-3 years
old who are inadequately immunized. During investigation, contacts are often treated
before the isolate’s serotype is known. MSDH requests that all Haemophilus influenzae
isolates be sent to the Public Health Laboratory (PHL) for serotyping.
Reporting Classification
Class 1.
Epidemiology and Trends
Prior to the development and widespread use of Hib conjugate vaccines in the late
1980’s and early 1990’s, Hib was the most common cause of bacterial meningitis in
children < 5 years of age. In Mississippi, conjugate vaccine was first offered to 18 month
olds in 1989, to 15 month olds in 1990, and as a primary series, starting at 2 months of
age, with a 12-15 month booster, in January 1991. With the institution of vaccination, the
number of reported cases of invasive disease dropped from 82 in 1989, to 5 by 1994.
There have been less than 5 cases per year since 1995.

34
In 2010, there were 15 cases of invasive disease due to Haemophilus influenzae
reported to MSDH. None of these reported cases of H. influenzae were determined to
be type b.
Hepatitis A
2010 Case Total
2
2010 rate/100,000
0.1
2009 Case Total
9
2009 rate/100,000
0.3
Clinical Features
Hepatitis A is a viral illness with an abrupt onset of fever, malaise, anorexia, nausea,
vomiting, and abdominal pain, followed by jaundice in a few days. The disease varies
in intensity from a mild illness of 1-2 weeks, to a severe disease lasting several months.
Most cases among children are asymptomatic and the severity of illness increases with
age; the case fatality rate is low—0.1%-0.3%. No chronic infection occurs.
Infectious Agent
Hepatitis A virus (HAV), an RNA virus.
Reservoir
Humans, rarely chimpanzees and other primates.
Transmission
Transmission occurs through the fecal-oral route either by person to person contact or
ingestion of contaminated food or water. Common source outbreaks may be related
to infected food handlers. Many younger children are asymptomatic, but shed virus
and are often sources of additional cases.
Incubation
Average 28-30 days, (range 15-50 days).
Period of Communicability
Infected persons are most likely to transmit HAV 1-2 weeks before the onset of
symptoms and in the first few days after the onset of jaundice, when viral shedding in
the stool is at its highest. The risk of transmission then decreases and becomes minimal
after the first week of jaundice.
Methods of Control
In the prevaccine era, hygienic measures and post-exposure immune globulin were the
primary means of preventing infection. Vaccine was first introduced in 1995, and

35
following successful vaccination programs in high incidence areas, the Advisory
Committee on Immunization Practices (ACIP) recommended routine vaccination for all
children in 2005. Children aged 12-23 months of age should receive one dose of
hepatitis A vaccine followed by a booster 6-18 months later, with catch up vaccination
for children not vaccinated by 2 years of age.
Post-exposure prophylaxis is recommended, within two weeks of exposure, for all
susceptible individuals who are close personal contacts of, or attend daycare with
infected individuals, or are exposed to hepatitis A virus through common source
outbreaks. Hepatitis A vaccine (with completion of the series) is recommended for
post-exposure prophylaxis for all healthy persons aged 12 months to 40 years. Immune
globulin should be considered for children less than 12 months of age, adults over 40
years of age, and those in whom vaccination is contraindicated. Use of both
simultaneously can be considered with higher risk exposures. Post-exposure prophylaxis
is not generally indicated for healthcare workers unless epidemiological investigation
indicates ongoing hepatitis A transmission in the facility.
Reporting Classification
Class 1.
Epidemiology and Trends
There were two hepatitis A cases reported in Mississippi in 2010. This was significantly less
than the nine cases reported in 2009 and the three year (2007-2009) average of eight
annual cases (Figure 19). Both cases were in adults over the age of 18 and neither was
related to a common source outbreak.

36
Figure 19
Hepatitis B, acute
2010 Case Total
34
2010 rate/100,000
1.1
2009 Case Total
32
2009 rate/100,000
1.1
Clinical Features
An acute viral illness characterized by the insidious onset of anorexia, abdominal
discomfort, nausea and vomiting. Clinical illness is often unrecognized because
jaundice occurs in only 30-50% of adults and fewer than 10% of children. Approximately
5% of all acute cases progress to chronic infection. Younger age at infection is a risk
factor for becoming a chronic carrier with 90% of perinatally infected infants becoming
chronic carriers. Chronic cases may have no evidence of liver disease, or may develop
clinical illness ranging from chronic hepatitis, to cirrhosis, liver failure or liver cancer.
Hepatitis B infections are the cause of up to 80% of hepatocellular carcinomas
worldwide.
Infectious Agent
Hepatitis B virus, a hepadnavirus.
Reservoir
Humans.

37
Transmission
Transmission occurs through parenteral or mucosal exposure to body fluids of hepatitis B
surface antigen (HBsAg) positive persons, such as perinatal exposure, through contact
with contaminated needles, or through sexual contact. Blood and blood products,
saliva, semen and vaginal secretions are known to be infectious. The three main groups
at risk for hepatitis B infection are heterosexuals with infected or multiple partners,
injection-drug users, and men who have sex with men.
Incubation
45-180 days, average 60-90 days.
Period of Communicability
As long as HBsAg is present in blood. In acute infections, surface Ag can be present 1-2
months after onset of symptoms.
Methods of Control
Routine hepatitis B vaccination series is recommended for all children beginning at
birth, with catch-up at 11-12 years of age if not previously vaccinated. The usual three
dose schedule is 0, 1-2, and 6-18 months. Vaccination is also recommended for high
risk groups, including those with occupational exposure, household and sexual contacts
of HBsAg positive individuals (both acute and chronic infections), and injecting drug
users.
Transmission of hepatitis B can be interrupted by identification of susceptible contacts
and HBsAg positive pregnancies, and the timely use of post-exposure prophylaxis with
vaccine and/or immune globulin.
Perinatal transmission is very efficient in the absence of post-exposure prophylaxis, with
an infection rate of 70-90% if the mother is both HBsAg and hepatitis B e antigen
(HBeAg) positive. The risk of perinatal transmission is about 10% if the mother is only
HBsAg positive. MSDH, through the Perinatal Hepatitis B Program, tracks HBsAg positive
pregnant women, provides prenatal HBsAg testing information to the delivery hospitals
when available, and monitors infants born to infected mothers to confirm completion of
the vaccine series by 6 months of age, and then tests for post-vaccine response and for
possible seroconversion at 9-12 months of age. Post-exposure prophylaxis is highly
effective in preventing hepatitis B vertical transmission, therefore, testing of all pregnant
women for HBsAg is recommended with each pregnancy.
Reporting Classification
Class 2.

38
Epidemiology and Trends
In 2010, 34 cases of acute hepatitis B were reported. This was comparable to the 32
cases reported in 2009, but lower than the three year average (2007-2009) of 44 cases
reported annually (Figure 20). Twenty-two (65%) of the 34 reported cases occurred in
individuals aged 15-34 years. There were five cases (15%) reported in individuals aged
40-45 years. Overall, the cases ranged in age from 15 to 44 years (Figure 21).
Figure 20
Figure 21

39
A comprehensive strategy to eliminate hepatitis B virus transmission was recommended
in 1991; it includes prenatal testing of pregnant women for HBsAg to identify newborns
that require immunoprophylaxis for prevention of perinatal infection and to identify
household contacts who should be vaccinated, routine vaccination of infants,
vaccination of adolescents, and vaccination of adults at high risk for infection.
In 2010, 46 HBsAg positive pregnant women were reported to the Perinatal Hepatitis B
Prevention Program (Figure 22). This was lower than the 82 reported in 2009 and the
three year average of 95. There were no reported cases of HBsAg positive infants born
to HBsAg positive mothers in 2010. This was similar to 2009 and 2008; however in 2007,
there were two cases of perinatal transmission.
Figure 22
HIV Disease
2010 Case Total
550
2010 rate/100,000
18.5
2009 Case Total
610
2009 rate/100,000
20.7
Clinical Features
The clinical spectrum of human immunodeficiency virus (HIV) infection varies from
asymptomatic infections to advanced immunodeficiency with opportunistic
complications. One half to two thirds of recently infected individuals have
manifestations of an infectious mononucleosis-like syndrome in the acute stage. Fever,
sweats, malaise, myalgia, anorexia, nausea, diarrhea, and non-exudative pharyngitis

40
are prominent symptoms in this stage. Constitutional symptoms of fatigue and wasting
may occur in the early months or years before opportunistic disease is diagnosed. Over
time, HIV can weaken the immune system, lowering the total CD4 count and leading to
opportunistic infections and the diagnosis of Acquired Immunodeficiency syndrome
(AIDS).
Infectious Agent
Human immunodeficiency virus is a retrovirus with two known types, HIV-1 and HIV-2.
These two types are serologically distinct and have a different geographical
distribution, with HIV-1 being primarily responsible for the global pandemic and the
more pathogenic of the two.
Reservoir
Humans.
Transmission
HIV infection can be transmitted from person to person during sexual contact, by blood
product transfusion, sharing contaminated needles or infected tissue or organ
transplant. Transmission by contact with body secretions like urine, saliva, tears or
bronchial secretions has not been recorded. Without appropriate prenatal treatment,
15-30% of infants born to HIV positive mothers are infected. Breast feeding is also a
known cause of mother to infant transmission of HIV.
Incubation
The period from the time of infection to the development of AIDS ranges from 1 year up
to 15 years or longer. The availability of effective anti-HIV therapy has greatly
decreased the development of AIDS among HIV infected individuals in the U.S.
Period of Communicability
Individuals become infectious shortly after infection and remain infectious throughout
the course of their lives.
Methods of Control
Abstinence is the only sure way to avoid sexual HIV transmission; otherwise mutual
monogamy with partners known to be uninfected and/or the use of latex condoms are
known to reduce the risk of infection. Confidential HIV testing and counseling and
testing of contacts, prenatal prevention by counseling and testing all pregnant women,
and treatment with appropriate anti-retroviral therapy can reduce transmission. Post-
exposure prophylaxis for health care workers exposed to blood or body fluids suspected
to contain HIV is an important worksite preventive measure. MSDH performs contact
investigation, counseling and testing for each reported case of HIV infection.

41
Reporting Classification
Class 1.
Epidemiology and Trends
Both HIV infection and AIDS are reportable at the time of diagnosis, so many patients
will be reported twice (once at first diagnosis of HIV infection, and again when
developing an AIDS defining illness). The epidemiologic data that follows is regarding
the initial report of HIV disease, whether first diagnosed as HIV infection or AIDS. Over
the past few years, there has been little change in HIV disease trends. There were 550
cases of HIV disease reported in 2010, an 8% decrease from 2006 (599) (Figure 23).
Figure 23
Individuals from every Public Health District were impacted by this disease. Public
Health District V reported the highest case rate, statewide, followed by District III (Figure
24).
2006 2007 2008 2009 2010
HIV Disease Rate (MS)
20.6 20.9 20.6 20.7 18.5
HIV Disease Cases (MS)
599 611 606 610 550
0.0
5.0
10.0
15.0
20.0
25.0
30.0
35.0
Incidence per 100,000 population
HIV Disease Rates by Year, Mississippi, 2006-2010

42
Figure 24
HIV Incidence by Public Health District, Mississippi, 2010
District
Cases
Rate*
I
56
17.5
II
42
11.6
III
50
23.1
IV
32
13.0
V
206
32.6
VI
30
12.3
VII
26
14.9
VIII
47
15.4
IX
61
13.1
State
550
18.5
*per 100,000 population
HIV disease was reported in all age groups, with 55% of the cases reported among 20-
39 year olds (Figure 25). African Americans were disproportionately impacted by HIV
disease. In 2010, 79% of new cases were among African Americans in which race was
known (Figure 26).
Figure 25
0
20
40
60
80
100
120
0-4 5-9 10-1415-1920-2425-2930-3435-3940-4445-4950-5455-59 60+
Number of cases
Age Group
HIV Disease Cases by Age Group, Mississippi, 2010

43
Figure 26
Additional References:
CDC. Guidelines for national immunodeficiency virus case surveillance, including
monitoring for human immunodeficiency virus infection and acquired
immunodeficiency syndrome. MMWR 1999/48(RR13;1-28.
Sterling, T. R. & Chaisson, R. E. (2005). General Manifestations of Human
Immunodeficiency Virus. In G. L. Mandell, J. E. Bennett, and R. Dolin (Eds.),
Mandell, Douglas, and Bennet’s Principles and Practice of Infectious Diseases (6
th
ed.). (Vols.1-2). (pp. 1548-1549). Philadelphia, PA: Elsevier Churchill Livingstone.
Influenza
Clinical Features
An acute viral infection of the respiratory tract characterized by sudden onset of fever,
often with chills, headache, malaise, diffuse myalgia, and nonproductive cough. The
highest risks for complications from seasonal influenza are in persons aged 65 years and
older, young children, pregnant and postpartum women, and persons at any age with
chronic underlying illnesses. Pneumonia due to secondary bacterial infections is the
most common complication of influenza. During the period 1976—2007, estimated
influenza deaths ranged from a low of 3,349 to a high of 48,614 per year in the United
States.
0
50
100
150
200
250
300
350
400
450
500
2006 2007 2008 2009 2010
Number of cases
Year
HIV Disease Cases by Race, Mississippi, 2006-2010
Black
White
Other

44
Infectious Agent
Influenza is caused by an RNA virus. There is usually one predominant subtype of
influenza virus causing the majority of infection each influenza season; however both
influenza A (H1N1 and H3N2) and influenza B have circulated each season.
Reservoir
Humans
Transmission
Transmission occurs person to person by direct or indirect contact with virus laden
droplets or respiratory secretions.
Incubation
The incubation period usually is 1 to 4 days, with a mean of 2 days.
Period of Communicability
From 1 day before clinical onset through 3-5 days from clinical onset in adults; and up
to 7-10 days from clinical onset in young children.
Methods of Control
Yearly vaccination is recommended with either trivalent inactivated vaccine (TIV) or
live attenuated influenza vaccine (LAIV). Education on basic personal hygiene,
specifically transmission from unprotected coughs and sneezes and from hand to
mucous membrane is highly important in preventing or slowing transmission of influenza.
Antivirals can also be used to prevent and treat influenza. The neuraminidase inhibitors
(oseltamivir and zanamivir), continue to be effective against all forms of influenza.
Fortunately, influenza A (H1N1) and A (H3N2), as well as influenza B viruses continue to
be sensitive to the neuraminidase inhibitors. High levels of resistance to the
adamantanes (amantadine and rimantadine) persist among influenza A (H1N1) and A
(H3N2) viruses circulating globally. The adamantanes are not effective against
influenza B viruses. Please consult the Centers for Disease Control and Prevention
(CDC), Prevention and Control of Influenza with Vaccines: Recommendations of the
Advisory Committee on Immunization Practices (ACIP), 2010. MMWR 59(No. RR-8);
August 6, 2010. http://www.cdc.gov/mmwr/pdf/rr/rr5908.pdf and the brief update
Prevention and Control of Influenza with Vaccines: Recommendations of the Advisory
Committee on Immunization Practices (ACIP), 2011. MMWR 60(33); 1128-1132; August
26, 2011. http://www.cdc.gov/mmwr/PDF/wk/mm6033.pdf
Reporting Classification
Class 1: Influenza-associated pediatric deaths (<18 years of age).

45
Epidemiology and Trends
Influenza activity usually occurs from December through March or April, but can occur
earlier or later. Peak activity typically occurs in February or March. The risk of
complications depends on many factors, including age and underlying medical
conditions. Vaccination status and the match of vaccine to circulating viruses affect
both the susceptibility to infection and the possibility of complications. Outbreaks can
occur in group settings, such as nursing homes.
MSDH monitors seasonal influenza activity statewide through an active syndromic
surveillance program reported by sentinel providers. In the 2010-2011 influenza season,
35 sentinel providers in 30 counties were enrolled in this system, representing hospital
emergency departments, urgent care and primary care clinics, and college and
university student health centers. These providers reported weekly numbers of
nontrauma patient visits consistent with an influenza-like illness (ILI), defined as fever
>100ºF and cough and/or sore throat in the absence of a known cause other than
influenza. MSDH uses this information to estimate the magnitude of the state’s weekly
influenza activity. These data are also used to estimate the geographic spread of
influenza within the state, ranging from no activity to widespread activity. This
terminology represents a geographic estimate rather than an indication of severity of
the season. ILI providers are also supplied with kits for PCR influenza testing at the Public
Health Laboratory (PHL).
The 2009-2010 influenza season was dominated by the pandemic strain of influenza A
(2009 H1N1). After the peak of activity during the late summer and fall of 2009,
influenza activity remained at a lower but still significant level until April 2010.
The 2010-2011 influenza season was mild. It began with increasing reports of influenza-
like illness reaching a peak in December (Figure 27). This portion of the 2010-2011
season was dominated by Influenza B. As the season progressed into calendar year
2011, the dominant virus shifted to Influenza A (H3N2), although some cases of Influenza
A (2009 H1N1) and Influenza B continued to occur (Figure 28).

46
Figure 27
Figure 28

47
Legionellosis
2010 Case Total
12
2010 rate/100,000
0.4
2009 Case Total
4
2009 rate/100,000
0.1
Clinical Features
Legionellosis is an acute bacterial infection that has two clinical syndromes;
Legionnaires’ disease and Pontiac fever. Both syndromes can present with fever,
headache, diarrhea and generalized myalgias. Those with Legionnaires’ disease
develop a non-productive cough and pneumonia that can be severe and progress to
respiratory failure. Even with improved diagnosis and treatment, case fatalities rates are
approximately 15%. Pontiac fever is a self-limited illness that does not progress to
pneumonia or death.
Infectious Agent
Legionella pneumophila (L. pneumophila), a gram negative bacillus with 18 serogroups.
L. pneumophila serogroup 1 is the most common serogroup associated with illness.
Reservoir
Legionellosis is a waterborne disease. The best conditions for growth of the bacteria are
warm water temperatures, stagnation, sediment and low levels of biocide.
Transmission
Airborne transmission occurs when water sources contaminated with L. pneumophila
are aerosolized. Common sources of outbreaks are potable water systems,
whirlpools/spas and cooling towers.
Incubation
Legionnaires’ disease — 2-10 days, most commonly 5-6 days.
Pontiac Fever — 5-72 hours, most commonly 24-48 hours.
Period of Communicability
Legionellosis is not transmitted person to person.
Reporting Classification
Class 2.
Epidemiology and Trends
In 2010, there were 12 reported cases of Legionnaire’s disease in Mississippi. There were
no deaths of Mississippi residents reported. On average, 2 infections have been

48
reported annually over the past 3 years (Figure 29). Cases ranged in age from 20 to 78
years. Five of these cases were outbreak associated, please refer to the “Events of
Public Health Significance” section on page 91.
Figure 29
Listeriosis
2010 Case Total
5
2010 rate/100,000
0.2
2009 Case Total
5
2009 rate/100,000
0.2
Clinical Features
A bacterial illness that in immunocompetent adults may present as an acute, mild
febrile illness. In the elderly, immunocompromised persons, diabetics, alcoholics and in
newborns, illness may present as meningoencephalitis and/or septicemia. The onset of
meningoencephalitis can be sudden with fever, intense headache, nausea, vomiting
and signs of meningeal irritation. Infected pregnant women may be asymptomatic or
experience only a mild febrile illness; however, infection during pregnancy can lead to
miscarriage or stillbirth, premature delivery, or infection of the newborn. The case
fatality rate is as high as 30-50% in newborns.
Infectious Agent
Listeria monocytogenes, a gram-positive, rod-shaped bacterium.

49
Reservoir
Mainly occurs in soil, forage, water, mud and silage. Animal reservoirs include domestic
and wild mammals, fowl and people. Asymptomatic fecal carriage is as high as 10% in
humans.
Transmission
Ingestion of unpasteurized or contaminated milk and soft cheeses, as well as
vegetables and ready-to-eat meats, such as deli meats or hot dogs. Unlike most other
foodborne pathogens, Listeria tends to multiply in contaminated foods that are
refrigerated. In neonates, infection can be transmitted inutero or by passage through
the infected birth canal.
Incubation
Variable, estimated median incubation is 3 weeks (range 3-70 days)
Period of Communicability
Mothers of infected newborns can shed the bacterium in vaginal discharges and urine
for 7-10 days post delivery. Infected individuals can shed the bacteria in their stools for
several months.
Methods of Control
Education for proper food handling and preparation. Avoid unpasteurized (raw) milk or
foods made from unpasteurized milk, such as soft cheeses, which can support the
growth of organisms during ripening. Consume perishable and ready-to-eat foods as
soon as possible after purchase, and cook hot dogs thoroughly before consumption.
These recommendations are especially important during pregnancy. MSDH
investigates all reported cases for rapid identification of common source outbreaks.
Reporting Classification
Class 2.
Epidemiology and Trends
There were five reported cases of listeriosis in Mississippi in 2010, which was comparable
to 2009 and with the average number of cases reported for the past three years. The
incidence rate in Mississippi has remained below national rates since Listeria was added
to the National Notifiable Disease List in 2000 (Figure 30).

50
Figure 30
There were no neonatal infections reported in 2010. The five reported cases ranged in
age from 3 to 89 years old. One death was reported in a 76 year old. None of the
infections were epidemiologically linked or associated with common source outbreaks.
Lyme Disease
2010 Case Total
0
2010 rate/100,000
0.0
2009 Case Total
0
2009 rate/100,000
0.0
Clinical Features
A tick-borne bacterial disease characterized primarily by a distinct “bull’s-eye” rash
(erythema migrans) in the early stage of the infection. The rash is present in up to 60%-
80% of patients. Accompanying symptoms may include malaise, fever, headache, stiff
neck, myalgias, migratory arthralgias and/or lymphadenopathy. In untreated patients,
chronic or late manifestations may include musculoskeletal symptoms (joint swelling or
chronic arthritis), neurological manifestations (aseptic meningitis, cranial neuritis, facial
palsy, rarely encephalomyelitis), and cardiac abnormalities (specifically 2nd or 3rd
degree atrioventricular conduction defects).
Infectious Agent
Borrelia burgdorferi, a spirochete.

51
Reservoir
Small mammals, mainly mice. Deer are efficient maintenance hosts and play an
important role in transporting ticks.
Transmission
Transmission occurs through the bite of an infected Ixodes scapularis tick (black-legged
tick). Nymphs are more likely to transmit disease, and they feed primarily on small
mammals. Studies indicate the tick usually must be attached 24 hours or longer to
efficiently transmit the bacteria. No person to person transmission or maternal fetal
transmission has been confirmed.
Incubation
2-30 days after tick exposure for erythema migrans, however, early infection may be
unapparent and patients may present weeks to months after exposure with late
manifestations.
Methods of Control
Avoid tick infested areas when possible. When unavoidable, use tick repellant and
measures to decrease tick exposure. After leaving tick prone areas examine body well
and remove any ticks. It is important to promptly remove any attached ticks; it is not
necessary to remove the head.
Reporting Classification
Class 2.
Epidemiology and Trends
Most cases occur in late spring and summer. Lyme disease is not considered endemic
in Mississippi, although the vector is present in the state. Since 2004 the number of
annual reported cases has ranged from 0-3. There were no confirmed cases reported
in 2010, but there were two cases in 2007.
Measles
2010 Case Total
0
2010 rate/100,000
0.0
2009 Case Total
0
2009 rate/100,000
0.0
Clinical Features
Measles is a highly contagious viral illness characterized
by cough, coryza, conjunctivitis
(3 C’s), fever, an erythematous maculopapular
rash, and a pathognomonic
enanthema (Koplik spots). Complications are seen more frequently in children younger

52
than 5 years of age and in adults 20 years of age and older. Diarrhea, pneumonia and
encephalitis are the most common complications seen. The risk of death is higher in
these age groups as well; the most common cause of death is pneumonia in children,
and acute encephalitis in adults. Subacute sclerosing panencephalitis is a rare
degenerative central nervous system disease that is thought to be due to persistent
measles infection of the brain, and typically presents approximately 7 years after initial
infection.
Infectious Agent
Measles virus, in the paramyxovirus family.
Reservoir
Humans.
Transmission
Transmitted by direct contact with large infectious droplets or, less commonly, by
airborne spread. Measles is highly contagious, and all persons without previous disease
or vaccination are susceptible.
Incubation
Eight to ten days.
Period of Communicability
Three to five days before to four days after rash onset.
Methods of Control
Measles, mumps and rubella (MMR) vaccine is recommended for all children at 12 to15
months of age with a second dose at school entry (4 to 6 years of age). Appropriate
two dose vaccination induces immunity in 99% of individuals.
MSDH investigates all reported cases and provides prophylaxis for all contacts as
appropriate. Measles vaccine administered within 72 hours of exposure may provide
protection in some cases. Immunoglobulin, given within six days of exposure, can
prevent or modify measles in susceptible persons who are at high risk for complications.
During 2001--2010, a total of 159 imported cases were reported in U.S. residents,
including 47 in children aged 6--23 months. Because measles remains endemic in
much of the world, international travelers should be up-to-date on vaccinations. In
accordance with the Advisory Committee for Immunization Practices (ACIP)
recommendations, U.S. children who travel or live abroad should be vaccinated at an

53
earlier age than those living in the United States because of the greater risk for exposure
to measles outside the United States, and particularly outside the Americas.
Reporting Classification
Class 1.
Epidemiology and Trends
Measles occurs throughout the world with peak incidence usually in late winter and
spring. There have been no reported cases of measles in Mississippi since 1992, when
there were 17 reported cases. Fifteen of those cases were associated with an outbreak
at the University of Mississippi and the index case’s infection in that outbreak was traced
to an exposure in Europe. Following this outbreak, a history of 2 doses of MMR was
required to attend public universities in Mississippi.
Widespread measles immunization has led to the interruption of endemic transmission
of measles in the United States and Mississippi. However, measles continues to be
endemic or has become endemic again in several countries, particularly in Europe, due
in part to dropping immunization rates. Sporadic outbreaks are reported in the U.S. and
are largely due to imported cases. Transmission from these cases easily occurs in
communities with high numbers of unvaccinated persons. Continued high vaccine
rates in the U.S. and in Mississippi are important to provide appropriate population
immunity and decrease the risk to those who are too young to receive vaccine or have
medical contraindications to vaccination.
Meningococcal disease, invasive
2010 Case Total
5
2010 rate/100,000
0.2
2009 Case Total
5
2009 rate/100,000
0.2
Clinical Features
Invasive meningococcal disease is an acute bacterial illness characterized by
meningitis and/or meningococcemia that may rapidly progress to purpura fulminans,
shock and death. Symptoms include rapid onset of fever, severe headache, stiff neck,
nausea and vomiting, and possibly a petechial rash. The case fatality rate, even with
the use of antibiotics and improved supportive measures, remains high at 8-15%. Long
term sequelae occur in 10-20% of survivors and include hearing loss and mental
retardation.

54
Infectious Agent
Neisseria meningitidis (N. meningitidis), a gram negative aerobic diplococcus. The most
common serogroups in the United States are B, C, W-135, and Y. Licensed vaccines are
not protective against serogroup B.
Reservoir
Humans. Up to 5-10% of the population may be asymptomatic carriers.
Transmission
Transmission of N. meningitidis is person to person by direct contact with respiratory
droplets from the nose and throat of infected individuals or carriers. Less than 1% of
colonized individuals will progress to invasive disease.
Incubation
The incubation period is 2-10 days, commonly 3-4 days.
Period of Communicability
Individuals remain contagious until meningococci are no longer present in nasal or
throat secretions, usually 24 hours after antibiotic treatment has begun.
Methods of Control
Vaccination and post-exposure prophylaxis are effective in preventing invasive
meningococcal disease. Routine vaccination with the quadrivalent meningococcal
conjugate vaccine (MCV4) is recommended for all children aged 11-12 years, children
aged 13-18 years not previously vaccinated, and any person aged 2-55 years with
increased risk for meningococcal disease (terminal complement deficiencies,
functional or anatomic asplenia, college freshman living in dormitories, and travelers to
countries in which N. meningitidis is hyperendemic or epidemic). Use of the
meningococcal polysaccharide vaccine (MPSV) should be limited to persons older
than 55 years of age, or used when MCV4 is not available.
MSDH investigates each reported case and provides prophylactic antibiotics (rifampin)
for household contacts and other appropriate close contacts. Health care workers are
not usually at risk unless there is direct contact with nasopharyngeal secretions (mouth-
to-mouth resuscitation).
Reporting Classification
Class 1.

55
Epidemiology and Trends
In 2010, there were five reported cases of invasive meningococcal disease. This is
comparable to the number of reported cases in 2009. Typically, over the last decade,
5-24 cases are reported annually in Mississippi (Figure 31). Nationally, infants less than 12
months of age have the highest incidence of invasive disease. In the U.S., rates of
disease decline in early childhood, increase during adolescence and early adulthood,
then decrease again in older adults. The 2010 MS cases ranged in age from 20 days to
92 years, with 60% of the cases being less than five years of age (Figure 32).
MSDH requests that all isolates be submitted to the PHL for typing. Two of the confirmed
cases in 2010 were typed as serogroup B. The serogroups for the other 3 cases were
unknown or not able to be subtyped.
In total, rifampin prophylaxis was provided for 23 contacts of a meningococcal disease
case in 2010; eight (35%) of which were less than 18 years of age. There were no
confirmed deaths reported in 2010 from meningococcal disease.
Figure 31

56
Figure 32
Mumps
2010 Case Total
0
2010 rate/100,000
0.0
2009 Case Total
1
2009 rate/100,000
0.03
Clinical Features
A viral illness with acute onset of fever, tenderness and swelling in one or more of the
salivary glands. Parotitis is the most common presentation, but asymptomatic infections
do occur. Symptoms typically resolve within 7-10 days. Orchitis in postpubertal males
and oophoritis in postpubertal females are the most frequent complications.
Infectious Agent
Mumps virus, in the paramyxovirus family.
Reservoir
Humans.
Transmission
Spread through airborne transmission or by direct contact with infected droplet nuclei
or saliva.
Incubation
About 16 – 18 days (range 14 – 25).

57
Period of Communicability
Three days before to four days after onset of symptomatic disease. Virus has been
isolated from saliva up to 7 days before and 9 days after onset of parotitis.
Methods of Control
Measles, mumps and rubella (MMR) vaccine routinely given at 12 – 15 months of age
with a second dose at 4 – 6 years. Immunization of susceptible contacts may be helpful
in prevention of infection.
Reporting Classification
Class 2.
Epidemiology and Trends
In Mississippi, there are typically 1-2 cases reported annually. In 2010, there were no
reported mumps cases, compared to one case in 2009.
Pertussis
2010 Case Total
106
2010 rate/100,000
3.6
2009 Case Total
80
2009 rate/100,000
2.7
Clinical Features
An acute bacterial disease of the respiratory tract distinguished by prolonged
paroxysmal coughing with a characteristic inspiratory “whoop.” There are three clinical
stages: catarrhal stage, paroxysmal cough stage, and a convalescent stage. Post-
tussive vomiting is common in the paroxysmal stage. Infants under 6 months of age,
vaccinated children, adolescents and adults often do not have whoop or paroxysms.
Pneumonia is the most frequent complication; the majority of fatalities occur in children
under 6 months of age. Adults and adolescents may have a mild illness which often is
undiagnosed, but serve as a source of infection for unvaccinated or incompletely
vaccinated children.
Infectious Agent
Bordatella pertussis, an aerobic gram negative rod.
Reservoir
Humans. Adolescents and adults are reservoirs for B. pertussis and are often the source
of infection in infants.

58
Transmission
Direct contact with respiratory secretions by airborne route, probably via droplets.
Incubation
Average 9-10 days. (Range 6-20 days).
Period of Communicability
Most transmissible in the catarrhal stage (which lasts about 1 week) and then during the
first 2 weeks after onset of paroxysmal cough, or a total of 21 days after symptom onset.
Communicability then gradually decreases and becomes negligible. Individuals are no
longer considered contagious after 5 days of antibiotic treatment.
Methods of Control
Vaccination and post-exposure prophylaxis are effective in preventing pertussis.
Pertussis vaccine is combined with diphtheria and tetanus toxoids (DTaP); the primary
series consists of four doses given between the ages of 2 months and 18 months, with a
booster at 4-6 years of age.
Pertussis immunity wanes 5-10 years after the booster vaccine, leaving adolescents and
adults more vulnerable to infection. A pertussis containing vaccine (Tdap) was recently
approved for the vaccination of adolescents and adults. Adolescents and adults
should receive a single dose of Tdap to replace a single dose of tetanus (Td).
MSDH investigates each reported case and provides prophylactic antibiotics
(erythromycin, azithromycin) for all household contacts where there is a child less than
one year of age or a pregnant woman in the last three weeks of her pregnancy in the
home.
Reporting Classification
Class 1.
Epidemiology and Trends
Among the diseases for which universal childhood vaccination is recommended,
pertussis is consistently the one that has the highest number of cases annually.
Susceptibility of unimmunized persons is universal.
In 2010, there were 106 reported cases of pertussis infections, but many more go
undiagnosed and unreported. This is higher than the 80 cases which were reported in
2009, but comparable to the 104 cases reported in 2008. The three year average for
2007-2009 was 147 cases (Figure 33).

59
Figure 33
Infants less than 1 year of age, who are at greatest risk for severe disease and death,
continue to have the highest reported rate of pertussis. Forty-one (39%) of the cases in
2010 were among children less than 1 year of age (Figure 34). No pertussis deaths were
reported in 2010.
Figure 34

60
Pneumococcal disease, invasive
Pneumococcal disease, invasive, children less than 5 years of age
2010 Case Total
19
2010 rate/100,000
0.7
2009 Case Total
28
2009 rate/100,000
1.0
Clinical Features
An acute bacterial infection with two clinical invasive syndromes: septicemia and
meningitis. Septicemia is the most common clinical presentation, with a case fatality
rate as high as 60% among the elderly. Pneumococcal meningitis has a case-fatality
rate of 30%, but may be as high as 80% in elderly persons. Symptoms of meningitis
include abrupt onset of high fever, headache, lethargy, vomiting, irritability, and nuchal
rigidity. It is the leading cause of bacterial meningitis in children less than 5 years of
age. Neurologic sequelae are common among meningitis survivors.
Infectious Agent
Streptococcus pneumoniae, a gram-positive diplococcus. Most strains causing severe
forms of disease are encapsulated; there are 90 known capsular serotypes.
Reservoir
The nasopharynx of asymptomatic human carriers. Carriage is more common in
children than adults.
Transmission
Droplet spread and contact with respiratory secretions.
Incubation
Unknown; probably short, 1-4 days.
Period of Communicability
Period of communicability is unknown, but it is presumed that transmission can occur as
long as S. pneumoniae occurs in respiratory secretions.
Methods of Control
Conjugate and polysaccharide vaccines are available for the prevention of
pneumococcal disease. The conjugate vaccine (PCV7) is approved for children
younger than 24 months of age and children 24-59 months of age at risk for invasive
disease. PCV7 is administered at 2, 4, 6, and 12-15 months of age. The polysaccharide
vaccine (PPV23) is recommended for all adults 65 years of age and older and any

61
person 2 years of age or older at high risk for invasive pneumococcal disease (chronic
disease such as cardiovascular disease, pulmonary disease or diabetes, and individuals
with cochlear implants).
Reporting Classification
Class 2; invasive disease in children less than 5 years of age and all antibiotic resistant
invasive disease.
Epidemiology and Trends
In 2010 there were 19 reported cases of invasive disease caused by S. pneumoniae in
children less than 5 years of age. This was comparable to the 28 reported cases in 2009
(Figure 35). Of these19 cases, 12 (63%) manifested as septicemia, 4 (21%) had
meningitis, and three (16%) had S. pneumoniae isolated from another sterile site. Ages
ranged from 4 months to 3 years of age. Twelve of the 19 invasive S. pneumoniae
cases were antibiotic resistant.
A total of 96 cases of invasive S. pneumoniae infections were reported in 2010. Thirty-six
(38%) of those cases were reported as antibiotic resistant, compared to 56 cases
reported in 2009. This total included 12 children less than 5 years of age. Of the 36
reported cases, 27 (75%) were septic, three (8%) had meningitis, and two (6%) had S.
pneumonia isolated from pleural fluid. The specimen source for four cases was not
noted. Reported cases of antibiotic resistant invasive S. pneumonia disease ranged in
age from 5 months to78 years, with a median age of 40 years (Figure 36).
Figure 35

62
Figure 36
Rabies
Clinical Features
Rabies is an acute fatal progressive disease that affects the central nervous system.
Early signs include anxiety, discomfort or paresthesia at the site of the bite of an
infected animal, primarily raccoons and bats in the U.S. Progression to symptoms of
cerebral dysfunction such as confusion, agitation, delirium, hallucinations, and insomnia
occurs within a few days of symptom onset. This is followed by generalized paralysis,
coma and death within 2 to 10 days.
Infectious Agent
Lyssavirus, family Rhabdoviridae; an RNA virus. Variants occur among animal species
and geographic location, but all of the members of the genus are antigenically
related.
Reservoir
Rabies has an urban and a wild cycle. The urban cycle (maintained by rabid dogs) has
been reduced greatly in the U.S., but carnivores (primarily raccoons, wild canids, and
skunks) and several species of insectivorous bats maintain the wild cycle in areas of the
U.S. Currently, only bats maintain the cycle in Mississippi.

63
Transmission
The most common mode of rabies virus transmission is through the bite of an infected
host. All mammals are susceptible to varying degrees. Transmission has also been
documented through organ transplantation, specifically corneal transplants, from a
donor dying of undiagnosed rabies.
Incubation
The incubation period can be up to six months or longer. The incubation period is longer
the farther away the bite is from the CNS.
Period of Communicability
Rabies is transmissible once it reaches the CNS and can be found in the salivary glands.
The animal is usually exhibiting abnormal behavior and other clinical signs by this time.
Methods of Control
The best method of control is prevention. Domestic animal rabies vaccination
programs, as well as pre- and post-exposure rabies vaccination in humans have
significantly decreased the human risk and deaths from rabies in the United States.
People who are bitten by animals that are known reservoirs of rabies exhibiting
abnormal behavior, such as unprovoked aggressiveness, increased drooling or paralysis
should be considered at higher risk, and consideration should be given to the use of
post-exposure vaccination.
Recommendations for preventing and controlling rabies in animals can be found in the
Compendium of Animal Rabies Prevention and Control, at
http://www.nasphv.org/Documents/RabiesCompendium.pdf.
Recommendations for prevention of rabies in humans can be found in the document
by the Advisory Committee on Immunization Practices (ACIP) entitled Human Rabies
Prevention—United States, 2008, at http://www.cdc.gov/mmwr/pdf/rr/rr57e507.pdf.
In 2009, the ACIP updated the guidelines for human rabies post-exposure prophylaxis.
These new guidelines were published in a March 2010 edition of the Morbidity and
Mortality Weekly Report (MMWR) entitled Use of a Reduced (4-Dose) Vaccine Schedule
for Postexposure Prophylaxis to Prevent Human Rabies - Recommendations of the
Advisory Committee on Immunization Practices
(http://www.cdc.gov/mmwr/PDF/rr/rr5902.pdf).
The following is a summary of these guidelines:
For immune competent individuals receiving first-time rabies post exposure
vaccine, the recommended series has been reduced from a series of 5 vaccine

64
doses administered on days 0, 3, 7, 14, and 28 to a series of 4 vaccine doses
administered on days 0, 3, 7, and 14.
ACIP recommendations for the use of Rabies Immune Globulin (RIG) remain
unchanged.
The number of doses recommended for persons who are immunosuppressed has
not changed.
Reporting Classification
Class 1 (human or animal).
Epidemiology and Trends
In the U.S. in the 1940s and 1950s, canines were the predominant reservoir and cause of
human rabies. By 2006, however, approximately 92% of animal rabies cases were in
wildlife, and only 8% were in domestic animals. This change is attributed to concerted,
targeted rabies vaccination campaigns and stray animal control that have reduced
the number of canine rabies cases from 6,947 in 1947 to 69 in 2010. Currently, most
human cases in the United States are caused by bat strains of rabies. In the U.S., skunks
and bats are now the most commonly reported rabid animal behind raccoons.
The MSDH PHL is the only laboratory in Mississippi that tests for rabies in animals. Since
1962, bats are the only animals that have tested positive for rabies in Mississippi. Usually,
between 2 to11 bats test positive each year. There were no positive bats out of 53
tested in the PHL in 2010. Since 2001, there has been a wide geographic distribution of
positive bats, with 51 reported positives in 25 counties (Figure 37). There has not been
an indigenous terrestrial animal (land) rabies case reported in Mississippi since 1961,
however, rabies occurs in terrestrial animals annually in states that border Mississippi
(Arkansas, Alabama, Louisiana, and Tennessee).
Mississippi reported a human case of rabies due to a bat strain in a 10 year old boy in
2005. Prior to this 2005 human case, the last reported human rabies case in Mississippi
was in 1953 and this was transmitted by a terrestrial animal.

65
Figure 37
Rabies in Bats by County, Mississippi, 2001-2010
Rocky Mountain spotted fever
2010 Case Total
27
2010 rate/100,000
0.9
2009 Case Total
9
2009 rate/100,000
0.3
Clinical Features
A rickettsial illness with acute onset of fever, severe headache, malaise, myalgia,
nausea, vomiting, and may include a macular or maculopapular rash on the
extremities, including the palms and soles, which usually spreads over the entire body.
A petechial rash often follows. In untreated cases and those with delayed recognition,
fatality occurs in 13-25% of the cases. Early stages of Rocky Mountain spotted fever
(RMSF) are often confused with ehrlichiosis and meningococcemia.
Infectious Agent
Rickettsia rickettsii, a gram-negative coccobacillus.
Reservoir
Small rodents (chipmunks, squirrels, white-footed mice).
County with at least one
positive bat

66
Transmission
Through bite of an infected Dermacentor variabilis tick (American dog tick). A 4-6 hour
attachment is required for transmission.
Incubation
3-14 days (most occurring between 5-7 days).
Period of Communicability
No evidence of person to person transmission.
Methods of Control
Avoid tick infested areas when possible. When unavoidable, use tick repellant and
measures to decrease tick exposure. After leaving tick prone areas, examine body well
and remove any ticks; removing the embedded head of the tick is not necessary.
Reporting Classification
Class 2.
Epidemiology and Trends
In 2010, there were 27 cases of Rocky Mountain spotted fever reported in Mississippi.
This is higher than the three year (2007-2009) average of 14 cases (Figure 38). The cases
ranged in age from 19 to 77 years of age. There were no reported deaths.
Figure 38

67
Rubella
2010 Case Total
0
2010 rate/100,000
0.0
2009 Case Total
0
2009 rate/100,000
0.0
Clinical Features
A mild, febrile viral disease characterized by a 3 day maculopapular rash. Children
often have few signs or symptoms other than the rash. The rash, typically fainter than a
measles rash, appears on the face initially and progresses distally. Adults may have a
febrile prodrome and lymphadenopathy. Up to 50% of all rubella infections are
subclinical or asymptomatic. Complications occur most often in adults and include
arthritis and encephalitis. Infection during pregnancy, especially in the first trimester,
may result in congenital rubella syndrome (CRS), causing fetal death, prematurity or
birth defects.
Infectious Agent
Rubella virus is classified as a togavirus, genus Rub virus.
Reservoir
Humans.
Transmission
Direct contact with nasopharyngeal secretions of infected persons or by droplet
spread. Rubella is moderately contagious. Maternal-fetal transmission causes CRS.
Incubation
Usually 14 days, with a range of 12-23 days.
Period of Communicability
The period of communicability is about 1 week before and up to 5-7 days after onset of
the rash. Infants with congenital rubella syndrome may shed the virus for months after
birth.
Methods of Control
Vaccination is the most effective method in preventing rubella. Rubella vaccine is
available combined with measles and mumps vaccines as MMR. The first dose of MMR
is recommended at 12-15 months, followed by a second dose at 4-6 years. All
susceptible adolescents and adults, especially women of child bearing age, should be
vaccinated with MMR vaccine.

68
Reporting Classification
Class 2.
Epidemiology and Trends
There were no reported cases of rubella in Mississippi in 2010. The last reported case in
the state was in a 4 year old in 1986.
Salmonellosis
2010 Case Total
1,215
2010 rate/100,000
40.9
2009 Case Total
901
2009 rate/100,000
30.5
Clinical Features
Salmonellosis is a bacterial disease that commonly presents as acute enterocolitis, with
sudden onset of headache, abdominal pain, diarrhea, nausea and sometimes
vomiting. Fever is almost always present. Dehydration may occur in infants and the
elderly, and septicemia occasionally results from infection.
Infectious Agent
Salmonella organisms are gram negative bacilli. The genus Salmonella is divided into
two species: S. enterica (divided into six subspecies) and S. bongori. Subspecies are
further divided into multiple serotypes. Almost all of the serotypes pathogenic for
humans are in one subspecies of S. enterica. Currently, there are more than 2460
identified Salmonella serotypes. The predominant isolates in Mississippi are Salmonella
serotypes Javianna, Mississippi, Newport and Typhimurium.
Reservoir
Domestic and wild animals, including poultry, swine, cattle, and rodents, and many
reptiles. Humans are also reservoirs, especially in mild and unrecognized cases.
Chronic carriers are prevalent in animals and birds.
Transmission
Salmonella is transmitted through ingestion of organisms in food derived from infected
animals or food or water contaminated by feces from an infected animal. Person to
person transmission by fecal oral route also occurs. S. serotype Enteritidis can be
passed trans-ovarially from infected hens to their eggs and transmission can then occur
when eggs are not fully cooked.
Incubation
From 6 to 72 hours, usually about 12-36 hours.
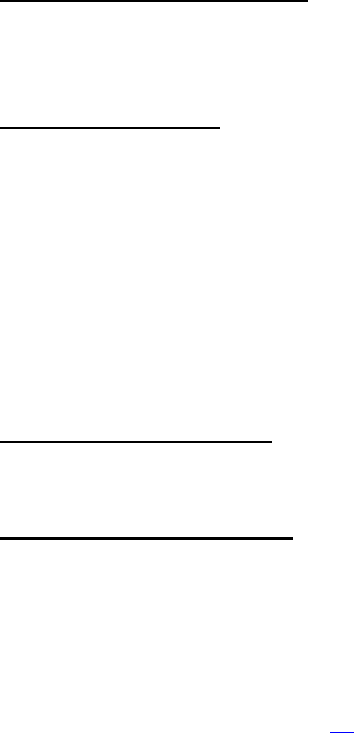
69
Period of Communicability
Throughout the course of infection; extremely variable, several days to several weeks.
A temporary carrier state occasionally continues for months, especially in infants.
Methods of Control
Transmission of Salmonella can be controlled with proper food preparation and sanitary
measures for food processing, proper hand hygiene, and clean water supplies. MSDH
investigates all possible common source food or waterborne outbreaks. The Public
Health Laboratory (PHL) requests isolate submission for molecular subtyping with pulsed-
field gel electrophoresis (PFGE). The DNA pattern, or “fingerprint”, is submitted to
PulseNet, a national tracking network coordinated by the CDC. This system facilitates
early detection of common source outbreaks, even if the affected persons are
geographically far apart, often allowing the source to be more rapidly identified.
Reporting Classification
Class 2.
Epidemiology and Trends
In Mississippi, 1,215 cases of salmonellosis were reported to MSDH in 2010. This marked
an increase in the rate and number of reported cases in Mississippi (Figure 39). In 2010,
the Salmonella serotypes Typhimurium, Newport, Mississippi, Enteritidis and Javiana
accounted for over 73% of the isolates seen in Mississippi. An outbreak of Salmonella
montevideo was identified in August 2010; please refer to the “Events of Public Health
Significance” section on page 93.

70
Figure 39
Infections occur in people of all ages, but there is higher incidence in infants and small
children. In 2010, 544 (45%) of the cases were in children less than 5 years of age (Figure
40).
Figure 40

71
Shigellosis
2010 Case Total
60
2010 rate/100,000
2.0
2009 Case Total
52
2009 rate/100,000
1.8
Clinical Features
An acute bacterial illness characterized by loose, often bloody stools (dysentery), fever,
and nausea with vomiting, cramps and tenesmus. Asymptomatic infections occur.
Illness is usually self-limited, lasting an average of 4-7 days; however infection with
Shigella dysenteriae (S. dysenteriae) is often associated with severe illness with a case
fatality rate of 20% among hospitalized patients. All age groups are susceptible, with
the peak incidence in 1-4 year olds. Children in daycares, persons in institutions, and in
facilities where adequate hand washing is difficult to maintain are at high risk for
outbreaks of shigellosis.
Infectious Agent
Genus Shigella, a gram negative bacterium comprising four serogroups: Group A, S.
dysenteriae; Group B, S. flexneri; Group C, S. boydii; and Group D, S. sonnei.
Predominant isolates in Mississippi are Group D, S. sonnei.
Reservoir
Humans are the primary reservoir.
Transmission
Primarily person to person by direct and indirect fecal oral contact. Infection may also
occur after ingestion of contaminated food or water. The infective dose can be as low
as 100-200 organisms.
Incubation
Ranges from 12 hours to 7 days, with an average of 2-4 days.
Period of Communicability
Until the agent is no longer present in feces. This is usually 4 weeks after cessation of
symptoms, but asymptomatic carriers may transmit infection for months or longer.
Methods of Control
Disease prevention includes promotion of good hand washing, exclusion from work for
food handlers or from school or daycare for children until symptom free for at least 24
hours. MSDH performs prompt investigation of common source food or waterborne
outbreaks, and investigates all reported infections in children less than 5 years of age.

72
Reporting Classification
Class 2.
Epidemiology and Trends
There were 60 cases of Shigellosis reported to MSDH during 2010, comparable to 2009
(Figure 41). There have been cyclic increases every 6-8 years since 1992, with a peak of
1,426 cases in 2007 associated with a large outbreak that occurred in the Jackson
metropolitan area and along the Gulf Coast. Although Shigellosis is usually a summer
month illness with 42% of the cases reported between May and August, cases are
reported to MSDH year round (Figure 42). The reported cases ranged in age from 10
months to 90 years, with 53% occurring in children less than 10 years of age (Figure 43).
Figure 41

73
Figure 42
Figure 43

74
Syphilis
Primary and Secondary Syphilis
2010 Case Total
229
2010 rate/100,000
7.7
2009 Case Total
224
2009 rate/100,000
7.6
Early Latent Syphilis
2010 Case Total
398
2010 rate/100,000
13.4
2009 Case Total
327
2009 rate/100,000
11.1
Clinical Features
Syphilis is a bacterial infection that has three stages: primary, secondary, and tertiary.
The primary lesion (chancre) is a painless indurated ulcer that develops at the sight of
initial infection, usually on the external genitalia. Even without treatment, this lesion
resolves in 4-6 weeks. Secondary syphilis may then develop and is characterized by a
generalized symmetrical maculopapular rash that often involves the soles and palms. It
may be accompanied by generalized lymphadenopathy, fever, malaise, sore throat,
headache and arthalgia. Clinical manifestations of secondary syphilis usually resolve
without treatment in weeks to months. Tertiary syphilis will develop years later in 15-40%
if untreated, primarily as cardiovascular or neurosyphilis, or as skin, bone, visceral or
mucosal surface gummas. Latent syphilis, a period of seroreactivity without clinical
disease, is classified as early (infection acquired within the preceding year) or late
(infection of more than a year’s duration).
Fetal transmission occurs through the placenta in untreated women with early syphilis,
resulting in congenital syphilis. Congenital syphilis can lead to abortions, stillbirths or
death shortly after birth. An infected infant may be asymptomatic for the first few
weeks of life; however, late manifestations may occur resulting in CNS involvement or
other conditions such as Hutchinson teeth, saddlenose, periostitis, interstitial keratitis or
deafness.
Infectious Agent
Treponema pallidum, a spirochaete.
Reservoir
Humans.

75
Transmission
Syphilis is transmitted primarily by sexual contact with an infected individual with early
syphilis (the first year of infection), especially during primary and secondary syphilis.
Transplacental infection of the fetus occurs during the pregnancy of an infected
woman, resulting in congenital syphilis. Transmission can also result from a blood
transfusion if the donor is in the early stages of infection.
Incubation
The average incubation period for syphilis before clinical manifestations is 3 weeks but
ranges from 3 – 90 days.
Period of Communicability
In untreated individuals, communicability can last for up to two years. Syphilis is most
communicable during the primary and secondary stages. Maternal-fetal transmission is
more likely in early syphilis, but may occur at any stage.
Methods of Control
Mechanical barriers, early detection, and effective treatment of the patient and their
partners are effective methods in prevention and control of syphilis. MSDH performs
contact investigation and treatment for each reported case of syphilis.
Reporting Classification
Class 1.
Epidemiology and Trends
Mississippi had a decline in primary and secondary (P&S) syphilis from 1997 through
2003, and since then has had an increase in rates. Although primary and secondary
(P&S) syphilis rates remained below the national average from 2002 through 2006, in
2010, MS ranked third nationally. In 2010, there were 229 reports of P&S syphilis, more
than double the number of cases reported in 2006 (Figure 44).

76
Figure 44
Districts IX and V had the highest incidence of P&S syphilis (Figure 45). Fifty-four percent
of P&S syphilis cases occurred among 20-29 year olds (Figure 46) and 85% of the cases
in which race was known were among African Americans (Figure 47).
Figure 45
Primary and Secondary Syphilis Incidence by Public Health District, Mississippi, 2010
District
Cases
Rate*
I
11
3.4
II
8
2.2
III
9
4.2
IV
11
4.5
V
81
12.8
VI
19
7.8
VII
4
2.3
VIII
24
7.9
IX
62
13.3
State
229
7.7
*per 100,000 population

77
Figure 46
Figure 47
Over the past ten years, Mississippi has had rates higher than national average for early
latent syphilis. Since 2004, there has been an increase in the number of cases, and in
2010, there were 398 cases of early latent syphilis reported (Figure 48).
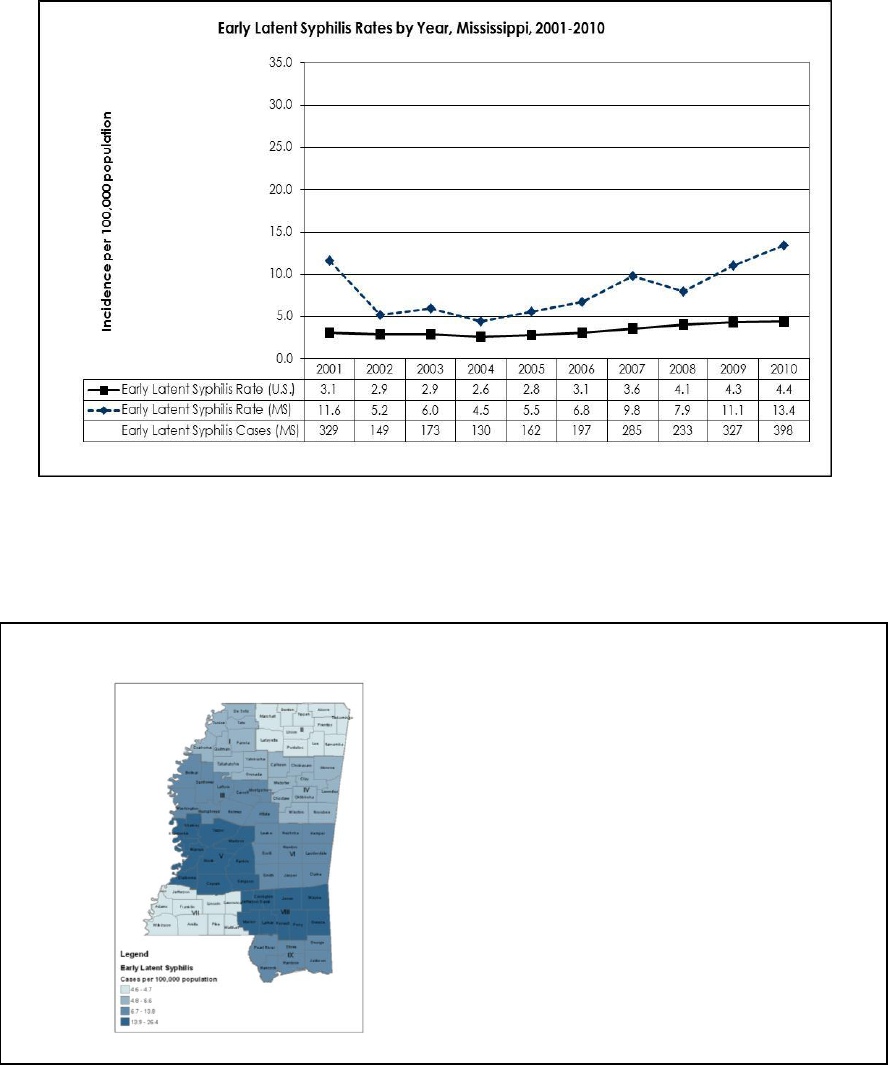
78
Figure 48
Early latent syphilis was reported in every district. District V and VIII had the highest case
rates in the state (Figure 49).
Figure 49
Early Latent Syphilis Incidence by Public Health District, Mississippi, 2010
District
Cases
Rate*
I
21
6.6
II
17
4.7
III
30
13.8
IV
14
5.7
V
167
26.4
VI
27
11.0
VII
8
4.6
VIII
57
18.7
IX
57
12.2
State
398
13.4
*per 100,000 population

79
Forty-three percent of reported cases were among 20-29 year olds (Figure 50). African
Americans are disproportionately affected, accounting for 85% of the cases for which
race was known (Figure 51) and had rates that were over twelve times greater than the
rate among whites.
Figure 50
Figure 51

80
Congenital Syphilis
Mississippi saw a decline in congenital syphilis cases reported from 1995 to 2004 and in
2005 and 2006, there were no cases reported. Congenital syphilis has reemerged since
2007 and there were 9 cases reported in 2010 (Figure 52). During this same time frame,
P&S syphilis cases among females doubled (from 35 to 69 cases).
Figure 52
Congenital syphilis was seen in five public health districts, with District VIII reporting the
highest rate.
Tuberculosis
2010 Case Total
116
2010 rate/100,000
3.9
2009 Case Total
121
2009 rate/100,000
4.1
Clinical Features
Pulmonary tuberculosis (TB) is the most common form of active TB disease; but, disease
can also be extrapulmonary and involve many organ systems. Symptoms are
dependent on the site of infection. Pulmonary TB generally presents with cough (dry
and later productive), pleuritic chest pains, hemoptysis, shortness of breath, fever,
malaise, weakness, night sweats, and anorexia and weight loss. Latent tuberculosis
infection without disease (LTBI) can occur and is asymptomatic.

81
Infectious Agent
Mycobacterium tuberculosis complex, an acid-fast bacillus.
Reservoir
Primarily humans, rarely primates; in some areas, diseased cattle, badgers, swine and
other mammals are infected.
Transmission
Exposure to tubercle bacilli in airborne droplet nuclei, 1 to 5 microns in diameter. The risk
of infection with the tubercle bacillus is directly related to the degree of exposure.
Incubation
A positive TB interferon gamma release assay (IGRA) result or TB skin test conversion,
indicating LTBI, occur 2-10 weeks after exposure to active TB disease, if infected. Ten
percent of persons with LTBI will develop clinically active disease, with the first 12-24
months after infection constituting the most hazardous period. HIV infection increases
the risk and shortens the interval for development of active disease following infection
with TB. In children, those under 5 years of age have the highest risk of developing
disease.
Period of Communicability
The degree of communicability depends on the number of bacilli discharged, virulence
of the bacilli, adequacy of ventilation, exposure of bacilli to sun or UV light, and
opportunities for aerosolization. Antimicrobial chemotherapy usually eliminates
communicability within 2-4 weeks. Young children with primary tuberculosis are
generally not infectious. LTBI is not infectious.
Methods of Control
Prompt identification, diagnosis, follow-up and treatment of potentially infectious
patients with TB disease are necessary to interrupt continued transmission. MSDH
performs contact investigations, TB targeted testing in high risk areas and provides
treatment for all active and latent TB infections.
Current Initiatives
A targeted testing program for the homeless population in Jackson was begun in late
2008. An IGRA test, Quantiferon-Gold, is provided to individuals seeking lodging/use of
the homeless shelters in the mid-city area. Annual testing is provided and an
identification card is issued and needed to access the shelters’ services. Over 1,000
persons have been tested and issued cards.
A pilot program for selected groups of latent TB patients using once-weekly doses of
Isoniazid and Rifapentene (3HP) was started in Hinds County and Public Health Districts
II, VIII and IX in July 2010. The treatment period is for 12 weeks and requires direct
observation of treatment.

82
Reporting Classification
Class 1.
Epidemiology and Trends
Mississippi had a consistent decline in TB morbidity from 1989 through 2005. TB rates
were below the national average in each of the 2001-2006 reporting periods. However,
from a low of 103 cases in 2005 and a high in cases in 2007 (137), reported cases have
leveled off during the past several years: 2008 (117), 2009 (121) and 116 in 2010. The MS
case rate continued to be above the national average in 2010, as it was in 2007 and
2009 (Figure 53).
Figure 53
Tuberculosis Rates by Year, United States and Mississippi, 2001-2010
0
1
2
3
4
5
6
7
8
9
10
Incidence per 100,000 population
TB Rate (US)
5.6
5.2
5.1
4.9
4.8
4.6
4.4
4.2
3.8
3.6
TB Rate (MS)
5.4
4.7
4.4
4.1
3.5
4.0
4.7
4.0
4.1
3.9
TB Cases (MS)
154
134
128
119
103
115
137
117
121
116
2001
2002
2003
2004
2005
2006
2007
2008
2009
2010
Geographically, TB was reported in every public health district, with the highest
incidence noted in Public Health Districts I and V (Figure 54).

83
Figure 54
Tuberculosis Incidence by Public Health District, Mississippi, 2010
Disease occurred across all age groups, with the majority in individuals 40 years old and
above (Figure 55). Disease in the African American population routinely accounts for
approximately two-thirds of morbidity (Figure 56). TB cases among patients co-infected
with HIV have increased since the beginning of the decade (Figure 57).
Figure 55
Tuberculosis Cases by Age Group, Mississippi, 2010
0
5
10
15
20
25
30
<1 1-4 5-9 10-
14
15-
19
20-
24
25-
29
30-
34
35-
39
40-
44
45-
49
50-
54
55-
59
60-
64
65+
Age Group
Number of Cases
District
Cases
Rate*
I
16
5.0
II
10
2.8
III
8
3.7
IV
9
3.6
V
44
7.0
VI
4
1.6
VII
5
2.9
VIII
12
3.9
IX
9
1.7
State
116
3.9
*per 100,000 population

84
Figure 56
Tuberculosis Cases by Race, Mississippi, 2001-2010
0
20
40
60
80
100
120
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010
Year
Number of cases
Black
White
Other
Figure 57
Tuberculosis and HIV Coinfections, Mississippi, 2001-2010
0.0
2.0
4.0
6.0
8.0
10.0
12.0
14.0
16.0
2001 2002 2003 2004 2005 2006 2007 2008 2009 2010
Year
Percentage of TB cases Coinfected with
HIV

85
Varicella
2010 Case Total
12
2010 rate/100,000
0.5
2009 Case Total
5
2009 rate/100,000
0.2
Clinical Features
An acute viral disease with primary infection (chickenpox) characterized by a
generalized pruritic rash that progresses rapidly from macules to papules to vesicular
lesions before crusting. The rash will be seen in various stages of development, usually
appears first on the head, and is more highly concentrated on the trunk rather than
extremities. Adults may have 1-2 days of fever and discomfort prior to rash onset, but
the rash is frequently the first sign of disease in children. Adults may have more severe
disease and have a higher incidence of complications (secondary bacterial infections,
pneumonia, aseptic meningitis and encephalitis). Herpes zoster is a localized
manifestation of latent varicella infection, with incidence increasing with age. Lesions
usually follow unilateral dermatomal patterns, but can be widespread or disseminated.
Postherpetic neuralgia occurs in up to 15% of zoster patients.
Infectious Agent
Varicella zoster virus, a member of the herpes virus group.
Reservoir
Humans.
Transmission
Person to person transmission by airborne droplet or direct contact with the lesions.
Indirect spread can occur through contact with articles freshly soiled by vesicular or
respiratory secretions. Maternal-fetal transmission also occurs. Susceptible contacts to
localized herpes zoster may develop chickenpox by direct contact with fluid from the
lesions, but respiratory transmission can occur in disseminated zoster.
Incubation
The incubation period is 14-16 days with a range of 10-21 days.
Period of Communicability
The period of communicability can be up to 5 days before onset of the rash (usually 2
days) and continues until all lesions are crusted (about 5 days).

86
Methods of Control
The live attenuated varicella vaccine is effective in preventing chickenpox. Routine
vaccination is recommended at 12 months with a second dose at 4-6 years of age.
Two doses of vaccine are recommended for all susceptible healthcare workers. The
vaccine can also be used to prevent disease, or at least modify severity of illness, in
susceptible persons if give within 3 days of exposure to an infected individual.
In 2006, FDA approved herpes zoster vaccine for persons 60 years of age and older.
Clinical trials indicate vaccine efficacy of 64%, with less severe disease in those who
developed zoster, and 66% less postherpetic neuralgia.
MSDH investigates outbreaks of varicella and vaccine is recommended after exposure
if there is no evidence of prior disease or vaccination. The vaccine is 70% - 100%
effective in preventing or attenuating disease if given within 72 hours of exposure.
Reporting Classification
Class 1; varicella infection, primary, in patients >15 years of age.
Epidemiology and Trends
In 2010, there were 12 reported cases of varicella infection in patients 15 years of age or
older. The cases ranged in age from 16 to 43 years. Nine of these 12 cases were
epidemiologically linked to two separate outbreaks. The three year average from 2007
to 2009 was 7 cases of varicella per year.
MSDH investigated two varicella outbreaks reported in 2010. Please refer to the “Events
of Public Health Significance” section on page 93.
Vibrio disease
2010 Case Total
8
2010 rate/100,000
0.3
2009 Case Total
11
2009 rate/100,000
0.4
Clinical Features
Several noncholera Vibrio species can cause illness in humans, usually wound infections,
septicemia or gastroenteritis. Vibrio vulnificus and Vibrio parahaemolyticus are the two
most frequently reported species in Mississippi.
V. vulnificus causes sepsis 12 hours to 3 days after ingestion of contaminated seafood,
usually raw oysters, especially among people with chronic liver disease, alcoholism, or
immunosuppression. These same groups are at risk for severe wound infections from
contact with coastal waters. V. vulnificus sepsis is characterized by fever, chills,
87
blistering skin lesions, shock and death. The case fatality rate is over 50% when
septicemia occurs.
V. parahaemolyticus infection typically causes gastroenteritis with watery diarrhea with
abdominal cramps, nausea, vomiting and fever; less commonly wound infections.
Infectious Agent
Anaerobic, gram-negative halophilic (salt requiring) bacteria found naturally in marine
and estuarine environments. Vibrio vulnificus and Vibrio parahaemolyticus are the two
most frequently reported species in Mississippi. Other species common to Mississippi are
V. mimics, V. holiday, and V. fluvial is. Nontoxigenic Vibrio cholerae serogroups (non-
O1/non-O139) are also reported.
Reservoir
Found free living in warm coastal waters, and in fish and shellfish, particularly oysters.
Transmission
Ingestion of the organisms in raw, undercooked, or contaminated fish and shellfish, or
any food or water contaminated with raw seafood. Wound infections with V. vulnificus
occur when wounds are exposed to estuarine waters.
Incubation
Median incubation period of 23 hours, with a range of 5-92 hours.
Period of Communicability
Not typically transmitted person to person.
Methods of Control
Seafood should be cooked adequately. Wounds exposed to seawater (either
occupational or accidental) should be rinsed with clean fresh water. All children and
immunocompromised individuals, especially alcoholics or individuals with liver disease,
should avoid eating raw seafood, especially oysters. MSDH investigates all reported
cases to determine the source of infection and possible risk factors of the case.
Reporting Classification
Class 2.
Epidemiology and Trends
In 2010, there were eight reported Vibrio infections. This was a slight decrease from the
number of reported cases in 2009 (11) and comparable to the three year average of 9
cases for 2007-2009 (Figure 58).

88
Of the eight reported cases, three were due to V. vulnificus (all isolated from blood
cultures), three were due to V. parahaemolyticus (two isolated from a stool culture and
the other from a wound), and two were due to V. mimicus (one isolated from stool
cultures and one isolated from a urine culture). There was one reported death
attributed to V. vulnificus in 2010, in a 79 year old man with an underlying history of
cirrhosis.
Figure 58

89
Events of Public Health Significance
This section of the Annual Summary of Selected Reportable Diseases reports on events
of public significance, including significant outbreak investigations conducted by the
Mississippi State Department of Health (MSDH).
Botulism Case
On April 15, 2010, the Mississippi State Department of Health (MSDH) Office of
Epidemiology received a telephone call from a Mississippi hospital requesting
information on Clostridium botulinum toxin testing on a 70 year old female with an
underlying history of multiple medical problems. She was admitted to the hospital
through the emergency department on April 10, 2010 with a one day history of slurred
speech, confusion, dizziness and lower abdominal discomfort. By April 13, 2010 she
developed full cranial nerve deficits with paralysis of the eye muscles, facial paralysis,
and upper extremity weakness, but retained some strength in her lower extremities. She
ultimately went into respiratory failure requiring ventilation. Based on her clinical
presentation of descending flaccid paralysis, the local physician notified MSDH to
facilitate Clostridium botulinum toxin testing. The Centers for Disease Control and
Prevention (CDC) was contacted for consultation regarding the potential testing of
clinical samples and release of botulinum antitoxin. The local physician was put into
contact with the CDC Botulism Officer to discuss the patient’s condition and treatment.
The District Health Officer and District Epidemiology staff were contacted to begin the
investigation. At the time, the patient was unable to give a food or exposure history.
District staff was able to locate and interview several family members. With the help of
family members, the District Epidemiology Nurse was able to obtain access to the
patient’s home to look for evidence of any foods posing a risk for botulism. The nurse
was quickly able to identify an opened jar of home canned beets on the kitchen
counter establishing a potential link to botulinum intoxication.
Both the CDC Botulism Officer and the local physician were informed of the discovery.
Within four hours of the initial call to MSDH, approval for the release of antitoxin was
obtained, and the infusion of antitoxin was begun within 11 hours of first notification.
Prior to the antitoxin infusion, serum and gastric content specimens were collected, and
along with the home canned beets, were sent to CDC for evaluation. Testing there
confirmed the presence Clostridium botulinum toxin type B in the canned beets and in
the serum sample. The District staff determined that the canned beets were given to
the patient by an elderly neighbor. The patient was given the beets two days prior to
the onset of her symptoms. A home visit to the neighbor determined that the neighbor
had canned beets and other vegetables that had been given to the neighbor’s son
and to the patient. All had been consumed previously with the exception of two

90
additional jars of beets discovered under the neighbor’s sink. These jars were disposed
of by MSDH.
The patient initially improved after the antitoxin infusion, but again developed
respiratory distress, likely due to aspiration, and required re-intubation and ventilation.
She was ultimately transferred to a restorative care facility on April 27, and is now
undergoing rehabilitation.
Brucellosis Cases
There were two reported cases of brucellosis in Mississippi in 2010. Until 2010, the last
reported human cases of brucellosis in MS were in 2003.
In 2010 MSDH investigated a case of brucellosis that occurred in a 44 year old man. On
June 11, 2010, the MSDH Public Health Laboratory confirmed a Brucella species on an
isolate submitted from a hospital laboratory. Further testing at the Centers for Disease
Control and Prevention (CDC) identified the Brucella species as Brucella suis. The
culture was from a knee aspirate obtained during arthrocentesis on June 2. The patient
had undergone arthroscopic surgery in April to repair a right knee meniscus tear from
an injury playing basketball. Twice during the month of May, he sought medical
attention to have fluid drawn from his knee. On June 2, he presented complaining of
“fever” in his knee and had an arthrocentesis and cultures of the fluid grew Brucella.
On June 11, a personal interview with the patient was conducted in order to obtain a
history of his illness and to identify a possible source of infection. He gave no history of
unpasteurized milk consumption. He did hunt and wrestle feral hogs and prepare the
hogs for processing. The exposure to feral hog tissue was considered a possible source
of infection. The patient was treated and recovered.
The MSDH also investigated the possible risk of exposure to Brucella in laboratory
employees that handled specimens or isolates. Consultation and guidelines published
by the CDC, Brucellosis: Description, Testing, Treatment, and Laboratory Risk Assessment
with Post-exposure Prophylaxis Recommendations for Exposure to Brucella spp.,
(http://www.cdc.gov/nczved/divisions/dfbmd/diseases/brucellosis/recommendations.
html) were referenced to identify, treat and monitor exposed persons. Possible
exposure occurred when biosafety recommendations were not used in the
manipulation of isolates. Plates were read and manipulated on an open bench (not
under a hood).
With the assistance of the hospital laboratory director and the infection preventionist,
twenty-eight laboratory personnel were identified as having potential exposure to the
bacteria. Three were identified with high risk exposure and twenty-five with low risk
exposure. All were offered post-exposure prophylaxis (PEP) with doxycycline and

91
rifampin and serological testing for Brucella at 0, 2 weeks, 4 weeks, 6 weeks, and 24
weeks post-exposure. All individuals exposed to Brucella isolates were to be actively
monitored for the development of symptoms weekly for six months after exposure. One
high risk laboratorian initiated PEP but stopped after two weeks of treatment due to side
effects. Sixteen potentially exposed laboratory personnel initiated blood testing.
Fifteen had three or more tests during the six month period. Seven had all five tests. All
were assessed for symptoms on a weekly basis.
On October 18, 2010, the MSDH was notified by the infection preventionist that a high
risk laboratory employee was reporting intermittent fever, malaise, and body aches.
This employee’s identified exposure was the reading and manipulation of the isolates
on the open bench. She had declined post-exposure prophylaxis when offered. She
had had regular, on time serum samples for serology that were negative. The last one
was on 8/17 and the final test was due on 11/28. A sample for serology was obtained
as well as blood cultures. The employee was started on treatment with doxycycline
and rifampin. The employee’s serology was greatly elevated and the blood culture
grew B. suis.
The MSDH identified another possible exposure from the handling of the blood culture
specimen obtained on the symptomatic laboratory employee. The laboratory had
been instructed to obtain the blood culture but not to plate the culture. A part-time
night employee was not aware of this and plated the culture. She was considered to
have had a high risk exposure and was offered testing and post-exposure prophylaxis.
She completed PEP, all serological testing was negative and she developed no
symptoms after 6 months. Two other employees were identified as low risk for exposure.
One declined all recommended follow-up. One declined PEP but had three serology
tests performed that were negative. Both low-risk employees were symptom free at six
months.
Legionella Outbreak
In June, 2010, the MSDH was made aware of a Legionella case potentially associated
with a hotel stay. An environmental inspection was conducted. In July, 2010, the MSDH
was notified of two out-of-state residents who had been diagnosed with Legionnaires’
disease that had traveled to Mississippi prior to their onset and stayed at the same hotel
as the initial case. The MSDH in conjunction with the CDC began a full scale
epidemiological and environmental investigation. Sixty environmental samples were
collected for culture. 295 interviews were conducted of hotel guests. A total of eight
Legionnaire’s cases, 5 from MS and 3 out-of-state, were identified, including one death.
Cases ranged from 31 to 61 years of age with the median age being 57 years.
Environmental sampling yielded six positive cultures for two separate strains of
Legionella from the cooling tower of the hotel. Additional monoclonal antibody (Mab)
testing and sequence based typing (SbT) of the clinical and environmental samples

92
found the clinical isolates to be identical to one of the two isolates obtained from the
cooling tower. The MSDH and CDC recommended remediation of the cooling system
be conducted in accordance with the American Society of Heating, Refrigerating and
Air-Conditioning Engineers (ASHRAE) Guideline 12-2000, Minimizing the Risk of
Legionellosis Associated with Building Water Systems. Follow-up testing at the facility is
ongoing.
Norovirus Outbreak
Norovirus has been implicated as the most common cause of outbreaks of
nonbacterial gastroenteritis. Infection typically results in a self-limited, mild to moderate
illness, lasting one to two days in most individuals, with clinical symptoms of nausea,
vomiting, diarrhea, abdominal pain and low grade fever. Transmission is through the
fecal-oral route, and outbreaks are common in closed group settings such as nursing
homes, hospitals, and ships. The virus is persistent in the environment and can be
transmitted person-to-person via either direct contact or contact with contaminated
inanimate objects, such as doorknobs. Almost any type of food that is contaminated
may serve as a vehicle for outbreaks. The incubation period is usually 24-48 hours after
exposure. Individual cases of norovirus infection are not reportable in Mississippi, but
any suspected outbreak is reportable as Class 1.
The Mississippi State Department of Health (MSDH) investigated a report of
gastrointestinal illness in several individuals who attended a conference held March 8-
12, 2010 in Mississippi. Eleven individuals were identified with an illness consistent with
norovirus infection, which was confirmed as norovirus genogroup GII by RT-PCR testing
in two persons. The investigation epidemiologically linked the illnesses to the
consumption of raw oysters harvested in Louisiana. Leftover oysters served at the
conference were obtained and sent to the FDA Gulf Coast Seafood Laboratory (GCSL)
in Dauphin Island, Alabama where they were found positive for norovirus GII.
Oysters are filter feeders and can efficiently concentrate viruses and bacteria from
contaminated water. Oysters have previously been implicated in the transmission of
norovirus gastroenteritis in Mississippi. In January 2009, and again in March 2009,
norovirus outbreaks were epidemiologically linked to the consumption of raw oysters
harvested near Pass Christian, Mississippi, resulting in the closure of that harvest area for
the remainder of the 2009 season.
The noroviruses isolated in the stool samples in the outbreak reported in 2010 were two
separate genotypes. Mixed outbreaks can occur and are usually explained by non-
point source contamination, such as sewage runoff. As a result of this investigation, the
Louisiana Department of Health closed the identified harvest area.

93
Salmonella Outbreak
In 2010 MSDH investigated a large outbreak of Salmonella montevideo in a restaurant.
On August 8, 2010, MSDH was notified by an Emergency Department of multiple
persons who were presenting with complaints of vomiting and diarrhea. History
obtained by the Emergency Department staff identified the restaurant as being a
common exposure.
A complete epidemiological and environmental inspection was conducted. Sixteen
cases were culture confirmed for Salmonella montevideo. Twelve additional cases
were epidemiologically linked to the restaurant. Environmental specimens were taken
and were also positive for Salmonella montevideo. Ill foodhandlers and improper
handling of food were identified as the most likely source of this outbreak.
Varicella Outbreak #1
This outbreak occurred May 24-June 10, 2010. The illness was characterized by a
generalized itchy rash and fever among inmates and staff at a correctional facility. A
clinical sample was obtained by MSDH staff. This sample was confirmed positive by
PCR for varicella virus by the MSDH Public Health Laboratory. All inmates in the
correctional facility pod where the first case was found were quarantined. All inmates
in the facility (329) and the correctional facility staff were assessed and monitored for
symptoms. Three inmates and 2 staff met the case definition for varicella.
Recommendations were made to facilitate the interruption of person to person spread.
Post exposure varicella vaccine was offered by the correctional facility to the inmates
and employees. Daily contact was maintained between the correctional facility and
the Health Department nurse.
Varicella Outbreak #2
This outbreak was reported on December 17, 2010 by a residential facility. The illness
was characterized by an itchy rash and fever in a resident at the facility. A clinical
sample was collected by MSDH staff. This sample was confirmed positive by PCR for
varicella virus by the MSDH Public Health Laboratory. Post exposure vaccination was
recommended for susceptible staff and residents. Recommendations were made to
facilitate the interruption of person to person spread. The facility obtained disease
and/or vaccine history for 147 employees. 116 susceptible residents received varicella
vaccine. Three residents and no staff members met the case definition for varicella.

94
Reportable Disease Statistics
Mississippi Reportable Disease Statistics
2010
Public
Health District
I
II
III
IV
V
VI
VII
VIII
IX
State Total
Sexually
Transmitted
Diseases
Primary & Secondary Syphilis
11
8
9
11
81
19
4
24
62
229
Early Latent Syphilis
21
17
30
14
167
27
8
57
57
398
Gonorrhea
606
438
867
449
1805
591
328
552
560
6,196
Chlamydia
2459
1732
2744
1707
5300
2029
1397
1993
2061
21,422
HIV Disease
56
42
50
32
206
30
26
47
61
550
Myco-
bacterial
Diseases
Pulmonary Tuberculosis (TB)
16
10
8
9
44
4
5
12
8
116
Extrapulmonary TB
0
1
1
3
5
1
0
4
0
15
Mycobacteria Other Than TB
36
35
27
24
137
31
20
19
57
386
Vaccine
Preventable
Diseases
Diphtheria
0
0
0
0
0
0
0
0
0
0
Pertussis
5
9
3
16
8
36
8
4
14
106*
Tetanus
0
0
0
0
0
0
0
0
0
0
Poliomyelitis
0
0
0
0
0
0
0
0
0
0
Measles
0
0
0
0
0
0
0
0
0
0
Mumps
0
0
0
0
0
0
0
0
0
0
Hepatitis B (acute)
0
10
2
4
9
0
1
3
5
34
Invasive H. influenzae b
disease
0
0
0
0
0
0
0
0
0
0
Invasive Meningococcal
disease
3
0
0
1
1
0
0
0
0
5
Enteric
Diseases
Hepatitis A (acute)
0
1
0
0
1
0
0
0
0
2
Salmonellosis
109
207
38
152
311
100
85
75
124
1215*
Shigellosis
11
4
11
6
10
4
4
3
7
60
Campylobacteriosis
16
17
5
5
27
10
8
15
24
128*
E. coli O157:H7/HUS
0
1
4
13
4
0
0
0
2
24
Zoonotic
Diseases
Animal Rabies (bats)
0
0
0
0
0
0
0
0
0
0
Lyme disease
0
0
0
0
0
0
0
0
0
0
Rocky Mountain spotted fever
0
5
3
10
4
2
0
0
3
27
West Nile virus
3
0
3
1
0
1
0
0
0
8
*Address unknown: Pertussis (3 cases), Salmonellosis (14 cases), Campylobacteriosis (1 case).

95
Mississippi;
Provisional Reportable Disease Statistics
November 2011
Figures for the current month are provisional
Public
Health District
State
Totals*
I
II
III
IV
V
VI
VII
VIII
IX
Nov
2011
Nov
2010
YTD
2011
YTD
2010
Sexually
Transmitted
Diseases
Primary & Secondary Syphilis
-
-
-
-
-
-
-
-
-
†
16
†
199
Total Early Syphilis
-
-
-
-
-
-
-
-
-
†
47
†
540
Gonorrhea
-
-
-
-
-
-
-
-
-
†
565
†
5,617
Chlamydia
-
-
-
-
-
-
-
-
-
†
1,802
†
19,613
HIV Disease
-
-
-
-
-
-
-
-
-
†
48
†
479
Myco-
bacterial
Diseases
Pulmonary Tuberculosis (TB)
0
0
0
0
2
0
1
0
2
5
12
63
90
Extrapulmonary TB
0
0
0
0
2
0
0
0
0
2
2
13
10
Mycobacteria Other Than TB
1
3
1
1
9
0
1
0
6
22
24
308
362
Vaccine
Preventable
Diseases
Diphtheria
0
0
0
0
0
0
0
0
0
0
0
0
0
Pertussis
0
0
0
0
2
0
0
0
0
2
30
40
101
Tetanus
0
0
0
0
0
0
0
0
0
0
0
0
0
Poliomyelitis
0
0
0
0
0
0
0
0
0
0
0
0
0
Measles
0
0
0
0
0
0
0
0
0
0
0
0
0
Mumps
0
0
0
0
0
0
0
0
0
0
0
3
0
Hepatitis B (acute)
0
0
0
0
1
0
0
0
0
1
1
44
32
Invasive H. influenzae b
disease
0
0
0
0
0
0
0
0
0
0
0
3
0
Invasive Meningococcal
disease
0
0
0
0
0
0
0
0
0
0
0
4
5
Enteric
Diseases
Hepatitis A (acute)
0
0
0
0
0
0
0
0
0
0
0
7
2
Salmonellosis
2
42
1
3
19
2
6
8
10
94
**
80
1304
1166
Shigellosis
1
0
1
0
39
1
0
5
4
51
9
213
53
Campylobacteriosis
0
0
0
0
0
0
0
0
0
0
13
65
125
E. coli O157:H7/HUS
0
0
0
0
1
0
0
0
0
1
13
10
24
Zoonotic Diseases
Animal Rabies (bats)
0
0
0
0
0
0
0
0
0
0
0
2
0
Lyme disease
0
0
0
0
0
0
0
0
0
0
0
3
0
Rocky Mountain spotted fever
0
0
0
0
0
0
0
0
0
0
3
12
26
West Nile virus
0
0
0
0
0
0
0
1
0
1
0
52
8
*
Totals include reports from Department of Corrections and those not reported from a specific District.
**
Address unknown for one case.
†
Data not available.

96
List of Contacts, Editors and Contributors
Office of the State Health Officer
601.576.7634
Mary Currier, MD, MPH
State Health Officer
Office of Communicable Diseases/Epidemiology
601.576.7725
Paul Byers, MD
Acting State Epidemiologist
Joy Sennett, MHS
Director
Immunization Program
601.576.7751
Tammy Clark, RN
Director
STD/HIV/AIDS Program
Nicholas Mosca, DDS
601.576.7723
Director
Tuberculosis Program
601.576.7700
J.M. Holcombe, MPPA
Director
Editors
Theresa Kittle, MPH
Epidemiologist
Office of Communicable Diseases/Epidemiology
Thomas Chester, MD, MPH
Career Epidemiology Field Officer (CEFO)
Office of Communicable Diseases/Epidemiology
Contributors
Cindy Allard, RN
Sheryl Hand, RN
Jannifer Anderson, RN
Kendra Johnson, MPH
Bruce Brackin, MPH
Peggy Oakes, RN, WHNP
Alisha Brinson, MS
Steve Quilter, MPH
Monique Drake
Wendy Varnado, MS
97
General References
Heymann D, ed. Control of Communicable Diseases Manual. 19th ed.
Washington, D.C.: American Public Health Association; 2008.
CDC. Epidemiology and Prevention of Vaccine-Preventable Diseases, 2009. 11
th
ed.
Pickering LK, ed. Red Book: 2006 Report of the Committee on Infectious
Diseases. 27
th
ed. Elk Grove Village, IL: American Academy of Pediatrics; 2006.
CDC. Sexually Transmitted Disease Surveillance 2009; November 2010.
CDC. Diseases and Conditions A-Z Index. Available o
http://www.cdc.gov/DiseasesConditions/az/a.html.
CDC. Case Definitions for Nationally Notifiable Infectious Diseases. Available
online at: http://www.cdc.gov/osels/ph_surveillance/nndss/phs/infdis2010.htm.
CDC. MMWR: Summary of Notifiable Diseases, United States, 2000-2009. Available
online at: http://www.cdc.gov/mmwr/mmwr_su/mmwr_nd/.

MISSISSIPPI STATE DEPARTMENT OF HEALTH
570 East Woodrow Wilson
Post Office Box 1700
Jackson, Mississippi 39216-1700
