Vernon Memorial Job Shadow & Work Experience Program
Dear Job Shadow/Work Experience Applicants,
Thank you for your interest in our Job Shadow / Work Experience Program! We look forward to having you on-site at
our facility!
The Job Shadow / Work Experience Program is a beneficial experience that will help educate and provide insight to
multiple careers within the healthcare setting. Use our Job Shadow / Work Experience Program to gain an in-person
perspective on multiple career paths within various healthcare fields. We are dedicated to making your experience
at Vernon Memorial Healthcare memorable and rewarding.
There are a few things you must accomplish prior to beginning your job shadow/ work experience. This informational
packet will highlight our policies and procedures as they relate to patient privacy. It includes information about
HIPAA (Health Insurance Portability and Accountability Act), which is a set of privacy regulations that all health care
providers are required to enforce. We, as health care providers, are very concerned about our patients’ privacy and
the security of their health care information. Our goal is to help you learn your role in regard to patient privacy and
security.
Please complete all of the forms in this packet. Applicants should allow at least two weeks for processing. There are
several places for your signature. Signing each of the forms means you understand the information and agree to keep
any learned information confidential.
Please direct any questions, and return all completed forms, to Kim Sellers, RN at [email protected]. Office hours are
Monday through Friday 8:00 a.m. - 3:30 p.m. Feel free to also call if you have additional questions: 608-637-4359.
We look forward to seeing you,
Kim Sellers, RN – Health Coordinator
List of Items to Complete or Review:
View the List of Current Available Areas to Shadow
Complete the Job Shadow / Work Experience Request Form
Review & Sign Job Shadow / Work Experience TERMS
Review & Sign Dress Code Policy
Review & Sign Confidentiality Agreement
Complete the Health Form
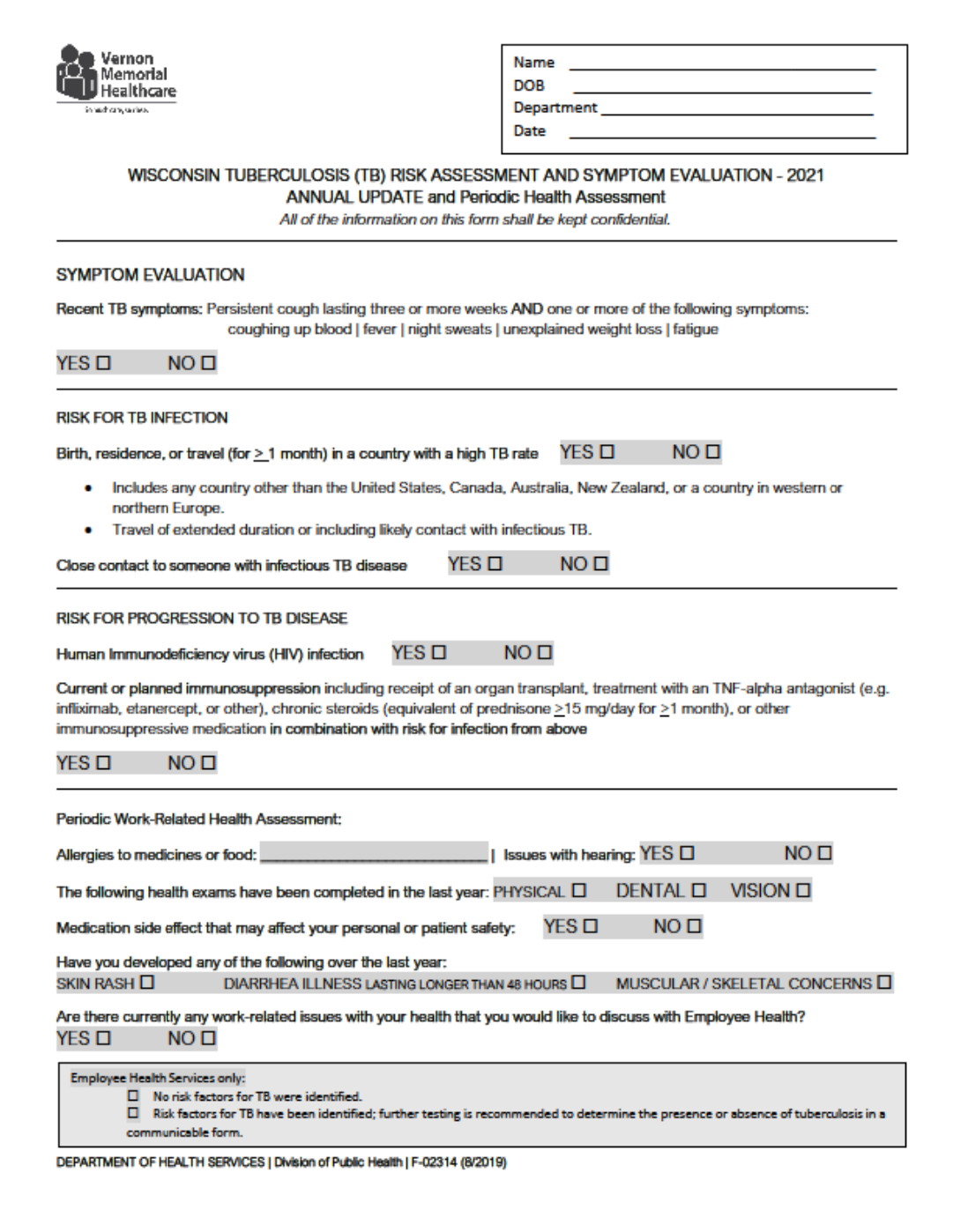
TB Risk Assessment Form (if no recent TB test)
Job Shadow Areas
(Subject to Change per Hospital Discretion)
Administration
Imaging (Radiology/X-ray)
Physicians
Anesthesiology
Information Systems (IT)
Physical Therapy
Business Office
Lab
Plant Services
Cardiac Rehab
Laundry
Public Relations and Marketing
Emergency Department
Nursing Dept. (Nurses/CNA)
Purchasing
EMT
Occupational Therapy
Respiratory Therapy
Environmental Services
Patient Accounts/Registration
Speech Therapy
Food and Nutrition Services
Patient and Family Services (Social
Work)
Surgery (Nurses, Physicians or
Surgery Techs)
Health Education
Pharmacy (Pharmacists) (Hospital
and Clinic Pharmacy)
Volunteer Services
HIS (Medical Records)
Pharmacy Techs
Other: Just ask us!
Human Resources
Physician Assistants
When requesting to job shadow a physician or practitioner, please be specific on what type of specialty you are
wanting to shadow. Example: general practice, pediatrics, emergency, surgery, etc.
If requesting to job shadow a nurse, please be specific on what type of specialty you are wanting to shadow.
Example: ER nurse, nurse who works with medical/surgical patients, nurse in a clinic, etc.
If you know the name of the person you would like to shadow in a specific department please indicate that on the
form as well. All attempts will be made to get you paired up with that person.
The more specific your request is, the better chance at getting an experience that will meet all of your expectations.
We will do our best to accommodate specific requests, but please note that staff availability, patient care, and
scheduling will take priority over job shadow / work experience requests.

Vernon Memorial Healthcare
Request for Work Experience Program
Reason For Request:
_____ Job Shadow-High School _____ Job Shadow-College _____ Work Experience _____ School to Work
_____ Other, Please Explain: ____________________________________________________________________
Department or Area of Interest: Days/Time Available:
1st Choice: ________________________________ Times Available: _________________________
2nd Choice: ________________________________ Days (circle all that apply): M TU W TH F
3rd Choice: ________________________________
Your Information (PLEASE PRINT CLEARLY):
Name:________________________________________ Phone Number: _______________________________
Address: _______________________________________________ Email: _________________________________
Date of Birth: ___________________ Gender (circle one): MALE FEMALE NON-BINARY OTHER: ___________
School you attend (if applicable): ___________________________________________________________________
School Contact Person (if applicable): __________________________________ Phone Number: ________________
Emergency Contact:
Name: ___________________________________________ Relationship: _________________________________
Primary Phone Number: _____________________________ Backup Phone Number: _________________________
HEALTH CONDITIONS & VACCINATIONS: Complete the required Health Form attached.
Any other comments or special requests: _____________________________________________________________
_______________________________________________________________________________________________
_______________________________________________________________________________________________
_______________________________________________________________________________________________
_______________________________________________________________________________________________
_______________________________________________________________________________________________
_______________________________________________________________________________________________

Job Shadow / Work Experience TERMS:
Job Shadow applicants must be at least 16 years of age or older.
Parent signature is required for applicants under the age of 18 years old.
Vernon Memorial Healthcare will not be responsible for transportation.
Vernon Memorial Healthcare will not be responsible for lost or stolen items (please only bring necessary
items into building).
Vernon Memorial Healthcare will not provide reimbursement for any cost associated with the job shadow /
work experience (gas money, time away from work, clothing, etc.).
Vernon Memorial Healthcare reserves the right to modify, change, or terminate this agreement at any time.
Vernon Memorial Healthcare reserves the right to end any job shadow / work experience during the
scheduled visit due to any reasons of concern such as safety, behavior, conduct, or breach of terms.
All packet requirements must be completed and turned in 2 weeks prior to shadow date.
Job Shadow / Work Experience requests must be approved by Kim Sellers, RN – Health Coordinator and the
department manager where visit will be conducted prior to a visit being scheduled.
Return all completed forms to [email protected]
I agree to the terms & conditions as required by this application:
______________________________________ _________________________
Applicant Name (PRINT) Date
______________________________________ _________________________
Applicant Signature Date
______________________________________ _________________________
Parental Name (PRINT) *Required if under age 18 Date
______________________________________ _________________________
Parental Signature *Required if under age 18 Date

Job Shadow Dress Code
The appearance of job shadow/work experience candidates at Vernon Memorial Healthcare has a direct impact on
patients’ and customers’ perceptions of our professionalism, competency and quality of care. All job shadow/work
experience candidates must adhere to general guidelines. Appearance must not be offensive to our patients and
staff.
Nametag (if applicable) must be worn visibly on the front of outer garments.
Hair must be clean and neat.
Personal Hygiene is important. Each job shadow/work experience candidate is expected to maintain good grooming
habits and hygiene to prevent body odor/bad breath. Limit the use of scented / fragrant products.
Clothing must be neat, clean, in good condition with proper fit. Tight clothing, low cut blouses or clothing that allows
undergarments to show through may not be worn. Skirts, dresses, shorts/skorts should be of moderate length.
Closed-toed shoes must be worn while job shadowing in any patient care area and for those who are involved in
lifting of objects or transfer of patients in any manner (wheelchair, cart, ambulating). Shoes should be kept clean, in
good condition, and reflect the needs of the work performed. *Business Office Setting: Sandals may be worn for visits
with non-patient care roles.
Accessories: Earrings, necklaces, rings etc. may be worn in moderation. Safety and patient care should be considered
when determining whether jewelry/accessories may be worn. Hats will not be worn indoors. No chewing gum is
allowed during patient contact.
*If the job shadow preceptor finds any clothing inappropriate or unprofessional, they reserve the right to cancel or
reschedule the job shadow, until appropriate attire is obtained.
I have read and understand the dress code requirements as indicated above:
Date: ___________________________________________________
NAME (PRINT): ______________________________________________
SIGNATURE: _________________________________________________

Confidentiality Agreement
Job Shadow/Work Experience
Vernon Memorial Healthcare (VMH) has a legal and ethical responsibility to safeguard the privacy of all patients and
to protect the confidentiality of their health information. Additionally, VMH must assure the confidentiality of its
human resources, payroll, fiscal, research, computer systems, and management information.
In the course of my job shadow / work experience at Vernon Memorial Healthcare, I may come into the possession of
confidential information.
By signing this document, I understand the following:
1. I agree not to disclose or discuss any patient, human resources, payroll, fiscal, research and/or
management information with others, including friends or family, who do not have a need-to-know.
2. I agree not to access any information, or utilize equipment without authorization and supervision, even
if I don’t tell anyone else.
3. I agree not to discuss patient, human resources, payroll, fiscal, research or administrative information
where others can overhear the conversation, e.g. in hallways, on elevators, in the cafeterias, on public
transportation, at restaurants, or at social events. It is not acceptable to discuss clinical information in public
areas even if a patient’s name is not used. This can raise doubts with patients and visitors about our respect
for their privacy.
4. I agree not to make inquiries for other personnel who do not have proper authority.
5. I agree not to willingly inform another person of my computer password or knowingly use another
person’s computer password instead of my own for any reason (if applicable).
6. I agree not to make any unauthorized transmissions, inquiries, modifications, or purging of data in the
system. Such unauthorized transmissions include, but are not limited to, removing and/or transferring data
from VMH’s computer systems to unauthorized locations, e.g. home.
7. I agree to log off prior to leaving any computer or terminal unattended (if applicable).
Date: ___________________________________________________
Print Name: ______________________________________________
Signature: _______________________________________________

Vernon Memorial Healthcare Job Shadow / Work Experience
HEALTH REQUIREMENTS FORM
Student Name:_____________________________________ School:______________________________________
Any Health Conditions? YES / NO If yes, please list:____________________________________________________
• The following immunization information are mandatory and must be completed in full.
• Copies of immunization records and/or lab results are needed to verify the information listed below:
please attach a COPY to this form.
MMR – Measles, Mumps, Rubella Vaccine:
2 MMR’s are required – or dates & results of Titers
Date of vaccine #1:__________, #2:__________
OR
Measles Titer Date:_________ Result:__________
Mumps Titer Date:_________ Result:__________
Rubella Titer Date:_________ Result:__________
Chicken Pox (Varicella) Vaccine:
Vaccine not needed if past history of having chicken pox.
History or disease: YES / NO
Date of vaccine #1:__________, #2:__________
OR
Varicella Titer Date:_________ Result:__________
Hepatitis B Vaccine:
3 Hep B vaccinations are required
OR a signed declination form.
Date of vaccine #1:__________
#2:__________
#3:__________
OR
Complete Signed Declination Form: ________________
TB Skin Test:
Negative TB skin test
OR complete TB Risk Assessment Form
Date of TB test:_________ Result:__________
_________ Result:__________
OR
Complete attached TB Risk Assessment Form: _____________
Flu Vaccine (November 1 – April 30):
Must have flu vaccination if job shadowing during above months.
Date of Flu Vaccine:_________________
COVID-19 Vaccine - MANDATORY
Brand: ______________ Dose 1: ____________ Dose 2: ____________
Health requirements and policies apply to all students coming for job shadow / work experience. It is the
student’s responsibility to submit accurate and timely information.
To the best of my knowledge, the above information is correct, and I do not currently have a communicable
disease or health condition that would put the patients/clients/staff or myself at risk.
_______________________________________________ ____________________________
Student Signature Date
_______________________________________________ ____________________________
Parent Signature (if student is under 18) Date