
The Cost Efficiency of Home Modifications to Reduce Healthcare Costs
Dr. Jesse M. Abraham*
Research Director
HomesRenewed Resource Center
For Presentation at the
Gerontological Society of America Annual Scientific Meeting
Phoenix, AZ
November 10-14, 2021
Abstract
The existing quantity of housing dedicated for older adults is not sufficient to meet the needs of
this growing population. And even as the Centers for Medicare and Medicaid Services
reimbursement structures are shifting from traditional inpatient and outpatient settings to care
in the home, it is a commonplace that most homes were not designed or built to support the
needs of aging residents or the provision of healthcare. It is time for America’s 100 million
existing houses to be made as safe and accessible as possible for aging in place. Falls cost over
$50 billion a year in medical expenses. This paper distills current knowledge regarding
healthcare cost reductions from home modifications, and then calculates the cost efficiency to
society and to the federal government of providing government subsidies for home
modifications for older adults at the ages of 50, 65 and 75. Cost sharing among insurers,
government and the beneficiary is one way to achieve the positive social returns.
*I would like to thank Louis Tenenbaum, who introduced me to this area of study and from
whom I have learned many of the ideas shared here. This paper has benefited by comments
from David Abraham and Louis Tenenbaum on an earlier version, but they have no
responsibility for any remaining errors.

1
Growing older at home has long been Americans’ overwhelmingly preferred housing option
(AARP, 2012) (AP-NORC, 2021).
1
Appropriately, the healthcare industry is preparing for a
future that includes the efficiencies of home-based care (Landers, 2016). But is the home safe?
According to the US Census Bureau’s 2019 American Housing Survey, of the 14(19) million
households headed by someone 75+(65-74), 46%(22%) had an acknowledged accessibility
problem (entering the home; getting to the bedroom, kitchen or bathroom; or using the
bedroom, kitchen or bathroom). Also see Molinsky (2020).
In this paper we show how the federal government might catalyze the widespread installation
of home accessibility features and save money doing it! As explained by Thaler and Sunstein
(2008), sometimes it can be sufficient to provide a ‘nudge’ in the direction of desired behavior.
2
This paper progresses through the following chain of logic to reach its conclusions. The existing
housing stock, which was built for a much younger population, is simply not ready to
accommodate the requirements of the evolving homeowner demographic. This outdated
housing stock becomes, literally, an accident waiting to happen when it comes to its
contribution to falls of older citizens. The installation of home accessibility features is uniquely
foundational in its ability to limit costly falls, while also bringing many other benefits. Within a
framework of the ‘Economics of Prevention’, a simple model is developed to derive the
healthcare cost/benefit of fall-prevention from home modifications. Model simulations
identify a cost-effective role for the federal government to subsidize the installation of
accessibility features for adults at the ages of 50, 65 and 75 years of age. With properly
designed programs the government can recover all of its subsidy, and more. The paper
concludes by reviewing limitations of this work and offering next steps for policy makers.
Where we are now
In recent years people have been turning to their homes to age in place in increasing numbers.
In part this is pure demographics: with steadily increasing longevity and the leading edge of the
Baby Boom generation having turned 65 in 2010, the population 65 and older is expected to
more than double from 35 million in 2000 to 73 million by 2030 (Howden (2011), Vespa (2018));
by 2035, a third of households are expected to be headed by someone who is aged 65+ (Joint
Center, 2019b).
Economically, many Americans have no choice but to age in place because they do not have the
financial resources to do anything else (Pearson, 2019). But the pandemic has also revealed
previously unappreciated risks of congregate care facilities (Mathews (2020), Economist (2020),
Inzitari (2020), Abrams (2021)). The Centers for Medicare and Medicaid Services (CMS) is
increasingly pivoting its reimbursement policies from traditional inpatient and outpatient
1
To limit the visual clutter, each citation in the text will provide only the first author’s name even when there are
multiple authors. All authors and document links are provided in the Reference list at the end.
2
The authors define ‘nudge’ as ‘any aspect of the (context in which people make decisions) that alters people’s
behavior in a predictable way without forbidding any options or significantly changing their economic incentives.’

2
settings towards care in the home (Pifer (2021), Holly (2020)); the healthcare industry is moving
towards a ‘hospital at home’ model (Piatkowski (2019), Leff (2021)).
AARP has been writing about the importance of updating one’s home since at least 1991
(Salmen, 1991). The National Home Modifications Action Coalition Blueprints report was
published in 1997 (Center for Universal Design, 1997). The MetLife Mature Market Institute
published its report on Aging in Place in 2010 (Tenenbaum, 2010) while the National Council on
Aging and Center for Disease Control and USC Leonard Davis School of Gerontology websites
all provide advice, practical information and serve as clearinghouses for information on state
and local programs.
3
4
Many existing elder care programs include home remodeling as part of
their recommendations; it is one of the three pillars of the widely embraced CAPABLE program
(Szanton, 2016).
The 2011 American Housing Survey included detailed questions on accessibility features and is
interpreted in Bo’sher (2015) and Will (2015). Ten years ago, 33% of all housing units had the
basic structural requirements of a stepless entry with a bathroom and bedroom on the main
floor, but only 4% of units had those features and were also equipped with no steps between
rooms or railings and grab bars; only 0.15% of all dwelling units were fully accessible to
someone in a wheelchair. The shares were closer to 40%, 10% and 0.6%, respectively, when the
sample is limited to households where someone has a disability. Ultimately, whether the
accessibility feature glass is half empty or half full depends on how well the need matches
reality on a house-by-house basis.
Half full? The 2011 National Health and Aging Trends Survey (NHATS) that samples specifically
households headed by someone at least 65 years old found that 61% of the respondents had at
least one accessibility feature to support bathing and toileting (Meucci, 2016). 20% of
homeowners over age 60 say they’ve made improvements to age in place (AARP, 2012) and
two-thirds of homeowners over age 55 say they consider themselves to be proactive in making
aging-in-place renovations (Cusato, 2016).
Or half empty? Over half of home service professionals indicate that aging-in-place projects
account for less than 10% of their work. Of those projects, up to a third are in reaction to
medical events which means the updates often must be made at the last minute while the
family is already coping with other healthcare needs (Cusato (2016), Joint Center (2019a)). Naik
(2005) identifies underutilization of environmental adaptations for bathing, while Lam (2021)
3
Many federal agencies provide programmatic and direct financial support of home remodeling for selected
groups in the community, including the Department of Veteran Affairs for veterans, the Department of Agriculture
for rural homeowners and the Department of Housing and Urban Development and the National Association for
Area Agencies on Aging for low-income elderly. Examples of published reports are HUD (2013), Stevens (2015),
Healthy Housing Solutions (2017), Convergence (2020) and Vespa (2020).
4
Australia created its Home and Community Care (HACC) program with its Home Modification and Maintenance
Services (HMMS) in 1985. See Jones (2008) and Public Health Administration (2019). The UK instituted the means-
tested Disabled Facilities Grants (DFG) program under the Housing Grants, Construction and Regeneration Act
1996. Its current annual budget exceeds £500 million. A program assessment is provided in Heywood (2001).

3
finds that of those individuals identified as having a problem in bathing and toileting in the 2015
NHATS, four years later in the 2019 survey 42% of those needs remain ‘unmet’. Admittedly it
can be challenging to assess the ‘true’ situation out there: Ahn (2011) find self-respondents’
assessment of the need for home modifications is heavily colored by their current home
satisfaction.
Aging in place has been demonstrated for many to be instrumental in preserving their quality of
life and supporting the social determinants of health (Carnemolla, 2018). For both family
pocketbooks and the federal government, extending time spent aging in place reduces
dependence on higher-cost congregate care facilities. And most easily quantified, home
modifications that enable safe aging in place can reduce the frequency and severity of falls,
directly saving healthcare dollars. Beyond altruism, it is in American society’s financial interest
to change the existing home modification delivery system.
Lessons can be learned from the market for residential solar panels, which in the last 20 years
have gone from upscale oddities to commonplace commodities. Unquestionably their embrace
has benefitted from technological advances and falling production costs. But generous
government subsidies have been part of a positive feedback loop, promoting and in turn
benefiting from higher societal demand for ‘green’ energy.
Fall Mitigation and Home Modifications
Falls are the leading cause of injuries and injury-related death for adults over the age of 65, in
America costing over $50 billion annually along with unquantifiable life changes and disruptions
(Collins, 2019). Truly a worldwide issue (WHO, 2008), there has for many years been extensive
development of fall mitigation interventions generating a deep literature around program
development and testing.
5
Systematic literature reviews (SLRs) seek to identify the salient results from programs that
include environmental screening for hazards, education, exercise and environmental
modification. The research varies extensively in sample population age, size, pre-existing
conditions, is typically combinations of interventions (multifactorial), experiences varying
degrees of subject follow-through on instructions, and has performance tracking of different
lengths of time and intensity.
Gillespie (2012) updates a 2009 Cochrane survey covering many kinds of fall intervention
studies; its 420 pages attest to its exhaustive breadth! They limit their scope to studies utilizing
5
The central role that housing features play in life quality and healthcare requirements is comprehensively
covered in WHO (2018). In this paper we are focused on the narrower issues of accessibility and fall prevention.
Specifically on these topics the WHO observes that ‘the certainty of evidence that home safety modification
programmes reduce the risk of injury was assessed as moderate, while … the certainty of the evidence that a
higher number of hazards in the home is associated with an increased risk of injury was assessed as moderate to
high’ (page 62).

4
the statistically rigorous random controlled trial (RCT) methodology and aggregate the results
of 159 separate studies covering 79,193 individuals. They find that many group-, home- or Tai
Chi exercise programs can be effective, reducing falls by 30%.
6
For home safety interventions
they find an average 30% reduction in falls and 20% reduction in the number of fallers; those
with a higher risk of falling were found to benefit more from the intervention.
7
As the vast majority of the time of elderly is spent ‘at home,’ the home is a natural place to
evaluate the person-environment fit (Gitlan, 2003). Professionally published papers citing
interventions identified as addressing ‘home safety’ or ‘environment modification’ can vary
widely in program design. Their intensity of home assessment can range from a single visit
from a government employee with a checklist moving identified hazards to multiple visits from
a team of medical, physical therapy, and occupational therapy (OT) professionals followed-up
with handyman services to make structural changes to the home. The timeframe for follow-up
can range from 2 months to 18 months. Results for the intervention cohort may be compared
with a control cohort of similar risk profile, or with the experience of the same cohort just prior
to the intervention, or even with a comparable population that just hasn’t yet received their
requested environment modification services from the state. The number of participants in
most of these studies are in the low hundreds – with one study having as low at 10 participants
– limiting their ability to deliver statistically significant results beyond a few primary questions.
8
Even as systematic literature reviews seek to make sense from the heterogeneity in test design,
they can become echo chambers that amplify the findings of a handful of papers, however truly
rigorous or comparable. Clemson (2008) summarizes results of 6 papers to conclude that there
can be a -21% reduction in falls from ‘environment interventions’, with a -39% reduction for
high-risk individuals (history of falling, functional decline, visual impairment). As they should,
the same 6 papers show up in Gillespie (2012). Pighills (2015) reaches the same conclusions as
Gillespie after reviewing 9 papers, seven of which were part of Gillespie’s sample. Stark’s
(2017) conclusions are broadly similar as well after reviewing 36 papers, though this paper
starts out by framing its question a bit differently, being to identify the ‘effectiveness of home
modification interventions within the scope of occupational therapy.’
The scoping review by Carnemolla and Bridge (2018) (referred to below as C&B) has a different
objective and one that aligns well with the focus of this paper. It finds 77 papers from 16
countries cataloging specifically home modification impacts and they go beyond fall reduction
to improved function; self-care or independence; physical health and well-being; caregiving;
economic effectiveness; ageing process; and social participation. This broader view is made
possible through not relying exclusively on RCT trials. The authors accept the limitations to
6
See Clemson (2004).
7
Gillespie (2012) also includes results from controlled interventions of medicine management, surgery,
psychological work, vision improvement and nutrition that do not concern us here.
8
There are also a growing number of programs being offered in the community that do not yet have the more
rigorous statistical results of academic studies. See North Carolina Housing Finance Agency’s Urgent Repair
Program, Baltimore’s HUBS program (IMPAQ, 2019), Detroit’s MHIS (Gaydayenko, 2020) and DC’s Safe at Home
program (Crowell (2017), Sheffield (2013)).

5
tight quantification of many of these impacts, citing the absence of single-factor studies of
specifically the home modifications and the imprecision across studies regarding what even
constitutes a ‘home modification.’
Quantification of Fall Reduction from Home Modifications
A formal systematic literature review selection process for this paper would inevitably have
been largely duplicative of the surveys already cited. This paper therefore embraces the
scoping review effort of C&B as its own. The paper review and selection process gone through
here starts with their compendium of 77 papers, while also including readings from other SLRs
cited as well as other relevant papers however sourced, as shown in Figure 1.
Our result is 20 papers, each of which are listed in Figure 2 along with summary information
about the study population, intervention and results, and the reported quantified results of the
intervention. These are all the original research papers, disintermediating literature reviews.
It is evident from the paper summaries that each one of these studies has a story of its own,
with not always clear quantified results on the contributions that the installation of structural
accessibility features makes to home safety. Very encouraging program results are reported in
Stark (2021) which focuses on hazard removal (the only site installation is grab bars/hand rails)
Starting Point:
Carnemolla and Bridge, 2018
77 papers in the review
C&B Papers Excluded
- 34 judged to be not relevant to this excerise
- 25 cited but not on home mod effectiveness
- 1 unable to find a copy
17 C&B papers quantifying
fall mitigation
5 additional papers found through other sources
3 papers listed in Figure 2 that support a primary
paper
Net 20 intervention results
quantifying the contribution
of home accessibility features
on fall mitigation
Flow Chart illustrating the Selection, Inclusion and Exclusion of Home
Modification Articles listed in Figure 2
Figure 1
6
for a 65+ population that recently had a fall or expressed fall anxiety. Their intervention costs
averaged $765.83 while generating health care savings in the 12-month assessment period that
amounted to $1613.63.
Some studies reviewed but not cited here included an OT-guided ‘home modification
assessment’ that remained vague regarding whether any structural modifications were made to
the property at all. Just to give a flavor of the diversity among studies that made the grade:
Keall’s ‘modifications’ included getting smoke detectors working, correcting inadequately
fenced driveways and reducing excessive hot water temperatures; Cumming’s largest
‘modification’ was removing dangerous floor mats; many of Cumming’s, Nikolaus’ and
Palvanen’s modifications were undone by the client during the evaluation period.
The Eriksen (2015) study most closely matches our use. Their clever design looks at the fall
reduction benefit from features installed in the home for the first-to-die spouse that accrue to
the surviving widow(er). Their data set is 1005 homeowners that are 65 and older in the
longitudinal Health and Retirement Survey who were recently widowed between 2000 and
2010. To control for the risk that the home features were installed for the survivor (which if
true would invalidate a foundational premise of this exercise), in their statistical work they use
the deceased spouse’s functional status as measured by ADLs as an instrumental variable for
the accessibility features. The safety and accessibility features are not singled out individually
but statistically treated as a group using a dichotomous variable (0/1) and may include: a ramp,
railings, modifications for a wheelchair, grab bars or shower seat, call system and ‘other
features.’ For those receiving the intervention, the study finds a -21.8% reduction in serious
falls for the whole population and a -38.6% reduction for individuals aged 75 and older. They
observe from their data that the ‘safety and accessibility features do not reduce overall fall
activity, but instead attenuate the severity of falls,’ that is they find a reduction in ‘serious’ falls
that incur expenses.
For our Baseline model simulation below we adopt the results of Eriksen: the installation of
accessibility features brings a 20% reduction in serious falls for individuals 65 and over and a
40% reduction for individuals 75 and over with chronic conditions. These numbers are
consistent with a scan of the final column of Figure 2. In fact, the consistency of the 20%/40%
results in that Figure is striking, even while each study may have a small sample size, quirks in
adoption rate, definition of ‘home mod’ and effort at behavior modification.

7
# Reference* Description Finding
1 Eriksen Population: #1005; 65+ mean age 75; in US -21.8% in serious falls
(2015) Intervention: track widower fall rates controlling for dead spouse's safety features -38.6% serious falls 75+
Results: no reduction in falls but significant reduction in serious falls
2 Tinetti Population: #301; age 70+ with risk factors; in US -24% fall reduction
(1994) Intervention: Medication review, behavior and exercise instruction, If nec grab bars, handrails, -31% falls per person-week
and raised toilet seat; 4.5mths of engagement
Results: fall reduction; cost of $12,392/fall requiring medical attention
3 Hornbrook Population: 3182; age 65+ mean age 73; in US -15% fall reduction
(1994) Intervention: removal of fall hazards, teaching, fitness classes, help installing bars 0% effect on injury falls
Results: reduction in falling, reduction in fallers, but not serious falls; tracking through 24m 0% effect on multiple falls
4 Plautz Population: #144; 60+ mean age 75; in US -59% in total falls
(1996) Intervention: VISTA worker with checklist; Avg $92.80 hardcosts and $50-100 labor
Results: Track 6mth prior and post intervention
5 Close Population: #397; aged 65+ mean age 78; selected post fall treatment in hospital; in Australia -61% in total falls
(1999) Intervention: Medical treatment, OT visit with checklist, move rugs; refer to govt for equipment -67% in recurrent falls
Results: 4,8,12m follow up; observe some falls b/c ice on pavement or external hazards 0% diff in serious injuries
6 Cummings Population: #530; 65+ with mean age 77; in Australia -19% in total falls
(1999) Intervention: most common is to remove floor mats; 50% compliance at 12 months
Results: only helped those with prior falls (-36%); conclude need OT to change behavior
7 Peel Population: #252; aged 51+ mean age 69; in Australia
(2000) Intervention: OT with checklist; renovations negotiated with govt services 0% change in falls
59% have atleast one mod to environment v 32% in control group
Result: reduced concern about falling; fall differences btwn groups all statistically insig
after 12m, -5% fall and -30% injurious fall; after 24m, +8% fall and +9% injurious fall
8 Salkeld Population: #530; aged 65+ mean age 76; in Australia
(2000) Intervention: OT with checklist; renovations installed with govt services -36% decline in falls for those
Mods: rug removal, nonslip bath mats, install handrails, pathway repairs, lighting with fall in previous year
Result: oddly find higher total medical costs for intervention Group
9 Stevens Population: #1737; aged 70+, RCT; in Australia
(2001) Intervention: home hazard assessment; free installation and education 0% change in falls
Results: 12m report window; no difference inside v out, around hazards or in total falls
10 Day Population: #1090; aged 70+; in good health; in Australia
(2002) Intervention: city staff labor use checklist and up to $54 to fix hand rails, floor coverings, etc 0% change in falls
Results: no fall reduction even though home hazards decreased from 10.2 to 7.4
11 Nikolaus Population: #360; mean age 82 with multiple chronic conditions; in Germany -31% in total falls
(2003) Intervention: home mods, OT, PT, social worker -37% for frequent fallers
Results: within 12 months many changes reversed; conclude need to change behavior -15% injuries
12 Liu Population: #9447; aged 70+; comparison of 2 waves of LSOA survey; in US -3.1% decline in physical
(2009) Intervention: track functional abilities of residents with varying mod install levels function
Result: 2yr report window; modestly greater functional decline without mods
13 Stark Population: #67; aged 60+ with mean age 82; in US 'improved' performance of
(2009) Intervention: pre/post compare with OT guided AT, safety mods and structural changes daily activities; 'reduced'
Results: 3m and 24m follow-ups; avg mod cost of $635 environmental press
14 Pighills Population: #238; age 70+ with fall history; RCT; in United Kingdom
(2011) Intervention: OT v Home Health worker guided enviro assessment and hazard removal unclear resuts
'where possible hazards were removed or repaired during 1-2 hr visit;'
Results: no reduction in fear of falling; -46% in falls in OT group; -22% insig fall drop in HH group
15 Mitoku Population: #547; age 65+ mean age 81; in Japan -48% mortality after 2 yrs
(2014) Intervention: install handrails, eliminate floor heights, change lavatory basin -35% mortality after 4.7 yrs
Results: fragility and mortality tracked at years 2, 3, 4.7
16 Palvanen Population: #1269; age 70+ at high risk; RCT trial at Fall clinic; in Finland -28% in total falls
(2014) Intervention: many services; 1 hr home visit with checklist, with home hazards 'reduced' -22% in fallers
Results: 12 month tracking period; home mod adherence was at 14% at 12 months -26% in fall-induced injuries
17 Szanton Population: #263; lower income; 65+ mean age 76; difficulty with 1 ADL or 2 IADLs; in US -30% in ADL disability score
(2014) &(2019) Intervention: CAPABLE which is OT, PT and $1222/client in home mod fixes Improved Quality of Life scores
Ruiz (2016) Results: 20 week tracking period; $22k/2yr savings to Medicare
Ruiz estimates a $22,000 net Medicare savings over two years
18 Kamei Population: #110, aged 65+ mean age 76; RCT; in Japan -14% falls of 75+ after 52w
(2015) Intervention: home hazard self modification after education session; grab bars only structure change -11% indoor falls of 75+
Results: 12w and 52w check-in; insig results for <75 year olds after 12 w
intervention group had 16-30% of identified hazards removed at 12w/52w check-ins
19 Keall Population: #842 mean age 43; people on govt subsidies; in New Zealand per person per year:
(2015) Intervention: Mean $450US spent fixing hazards and safety issues assessed by builders -26% in injuries caused by falls
Results: 3 year observation -39% in home mod related falls
Efficacy challenged in Robinovitch (2015)
20 Stark Population: #310; aged 65+ mean age 75; RCT with AAA clients in US No reduction in # of fallers
(2021) Intervention: OT-guided home hazard removal: grab bar installation, adaptive equip, task mod -38% in total falls
Results: After 12 months; achieve 90+% compliance; find avg $765.83 cost with $1613.63 savings No change in other 2nd outcomes
* Only first author. All interventions identified in Carnemolla and Bridge (2018) and in many other SLRs, with the exception of Eriksen (2015), Stark (2021) and Hornbrook (1994)
Figure 2
Fall Reductions from Home Modifications

8
This is not to discount the legitimate concerns of Keall (2015) and Cummings (1999) that it may
be more the person than the environment that needs the modification: the introduction to the
home of accessibility improvements without some behavior modification would clearly achieve
nothing.
9
Rather we’d suggest that the consistency across study results points to there being a
likely wide variety of methods for achieving behavior modification that are not limited to
training from occupational therapists. The consistency in finding a larger effect for
interventions for people with prior falls – perhaps they are more receptive to the message –
may be a reminder that for change to be sustained it needs to be embraced by the client and
not imposed from the outside. In the Eriksen study, the old-dogs may have learned their new
tricks by watching their (now deceased) spouse utilize the home accessibility features.
A Framework for Evaluating Home Modifications
A central thesis of this paper is that expenditures to update homes with accessibility features
should be recognized as cost effective healthcare prevention. But proving that is a tough
mountain to climb because true prevention means incurring costs for many who may ultimately
never benefit from the intervention. (And while not a problem with the intervention proposed
in this paper, many medical interventions can be accompanied by negative side-effects.)
Congressional Budget Office (2020) states that 80% of prevention spending improves
healthcare but on net, increases costs.
10
That only 20% of prevention spending is deemed cost
effective in part reflects CBO’s specific methodology which uses a 10-year window for
discounting expenditures and savings, incorporates only federal government expenditures and
savings, and seeks to incorporate all secondary impacts on federal spending -- noting in
particular any cost shifting towards the federal government such as incremental healthcare
spending that results from delayed mortality.
The CBO acknowledges that even if only 20% are cost effective according to their criteria, a
higher 60% of prevention spending produces clinical benefits that the research community
considers reasonable. Typically, research conclusions are reached through derivation of an
incremental cost effectiveness ratio (ICER) of dollars per quality adjusted life year (QALY) or
disability adjusted life year (DALY). That approach to evaluating home modifications is
discussed in a later section; the modeling focus in this paper embraces the CBO approach.
9
As noted in Lord (2006), there is a complex interaction between capability and environment, with the existence of
hazards not equating to realized falls. For example, more active individuals may take greater risks and hence
experience greater falls than frail individuals. Lord concludes the greatest home modification benefit comes to
those with a history of falls and mobility limitations.
10
See (Carroll, 2018).

9
Expenditures to prevent or reduce healthcare spending can be usefully characterized as falling
into one of the three stages shown in Figure 3 labeled primary, secondary and tertiary
(Academy Health, 2013). Cost versus benefit calculations will be unique to each of the three-
stages as conditions vary with how tightly each population is identified, treatment side effects,
false positive results and the duration of effectiveness:
• Tertiary prevention treatment (P3) applies to those individuals who are of particularly
advanced years (here taken to be 75 years old), have a history of falls, may have
multiple chronic conditions, and may be limited in their ADLs or IADLs. We think of this
group as being conceptually comparable to the CAPABLE study population.
• The secondary prevention population (P2) is considered to be all 65+ year olds who have
now aged into being ‘at risk’ for needing accessibility improvements and who are all
covered by federally-sponsored Medicaid or Medicare healthcare insurance.
• Finally, we consider the primary prevention population (P1) to be those individuals who
could choose to install accessibility features in their home even while being years away
from actually ‘needing’ them themselves. Over half of home remodeling expenditures
are made by households headed by someone aged 50+ (Joint Center, 2021), so this is a
population ripe to be incentivized to add accessibility features.
The populations we’ve described that fit into these groups are Americans at the ages of 50+,
65+ and 75+, respectively. For simplicity in the simulation work below we focus on the age
cohort that in the year 2020 turned 50, 65 or 75.
Primary Secondary Tertiary
Prevention Conceptual
Structure*
Measures intended to prevent the
onset of a condition
Measures intended to detect disease in
clinically asymptomatic people at an
early stage when it is most treatable.
Measures to slow the progression of a
disease after it is clinically obvious and
a diagnosis established.
As applied to modifying
a home with
accessibility features
This is the broad population with
undiagnosed needs but, if they live
long enough, will eventually 'age-
in' to needing accessibility features
to keep safe.
Individuals of advanced age are at risk
of needing accessibility features.
Established fall-risk individuals. Likely
of advantaged age, may have fallen
previously, may have multiple chronic
conditions.
Conceptually in the
Model
Households headed by someone
age 50+ who is planning to
renovate their home and might
consider including accessibility
features in their scope.
Households headed by someone age
65+ who is covered by federal health
insurance (Medicaid or Medicare).
Households headed by someone 75+
who is already 'disabled'.
Conceptually this is comparable to the
CAPABLE study population.
In the Model Simulation
P1. The 1.36 million households
headed by someone who turns 50
in 2020 that do not already have
accessibility features installed in
their home.
P2. The 1.50 million households
headed by someone who turns 65 in
2020 that do not already have
accessibility features installed in their
home.
P3. The 200,000 households headed by
someone who turns 75 in 2020 who is
identified as 'disabled' in the American
Housing S urvey.
* Academy Health (2013)
Figure 3
The Three Stages of Prevention

10
A Model of Cost Savings
A straightforward Excel model of the cost effectiveness of home modifications has been
developed for this paper.
11
Model inputs for the P1, P2 and P3 prevention Baseline scenarios
are shown in Figure 4. This aging model starts with a given population of owner-occupied
households (2020’s 50 year-olds, 65 year-olds or 75 year-olds with a disability in lines 1-3),
modifies all of their homes spending line 14, and plays-out the effects on falls (lines 7-10) being
reduced (or not) in every subsequent year of their lives while they remain in the same property.
The population at the start of each subsequent year is the prior year figure less move-outs and
deaths (lines 4-5). We run each simulation until the (initially) 50-, 65- or 75-year old reaches
the arbitrary age of 90. At that point an individual in each cohort has a 20-25% probability of
remaining alive and in their original residence; for federal government cost-effectiveness
calculations the meaningful time period is just the first 10 years. To make our calculations we
need data on the healthcare system cost of serious falls (line 11) and fatal falls (line 12) and the
percent reduction in falls from the home improvement intervention (line 16).
The baseline simulations assume the government absorbs all of the accessibility modification
costs (100% in line 18). That proves to be too large a share to be cost effective – even with a
11
A conceptually similar approach is undertaken in Smith (1998) for a population close to our P3. They construct a
decision tree model, populate transition rates sourced from an OT consultant and published sources, and adopt a
home mod fall reduction of -25% based on Tinetti (1994). With inputs of $172 in home modification costs and
$17,208 fall injury costs, they find a net savings of $92 per person (all in 1996AUS$) in their ten-year simulation.
P1 P2 P3
Population
Population 1 1,491,868 1,759,036 1,250,747
Population share eligible 2 100% 100% 28%
Share needing home mod 3 91% 85% 57%
Moves and Deaths
Annual Move-out rate (Avg) 4 0.82% 1.48% 1.73%
Annual Mortality rate (Avg) 5 1.35% 5.33% 7.46%
Life expectancy (years @ start) 6 31.45 19.17 12.03
Fall Rates
Annual fall rate (Avg) 7 11.42% 30.20% 32.80%
Serious falls share of annual falls (Avg) 8 15.37% 36.80% 37.20%
Serious fall rate creating costs (Row7*Row8))
9 1.75% 11.11% 12.20%
Fatal fall rate of population (Avg) 10 0.013% 0.070% 0.105%
Fall Costs
2020 cost of serious falls ($000) 11 11.499 11.499 11.499
2020 cost of fatal falls ($000) 12 30.972 30.972 30.972
2020 per capita healthcare spending ($000) 13 22.765 22.765 22.765
Home Improvement
Cost of home improvement ($000) 14 4.400 4.400 4.400
Baseline annual rate of home mods 15 2.5% 2.9% 4.3%
Fall reduction from intervention after age 65 16 -20% -20% -40%
Fall reduction effectiveness in year 5 17 100% 100% 100%
Financial
Government share of Home Mod cost 18 100% 100% 100%
Government share of medical costs 19 75% 75% 75%
Medical cost inflation rate 20 3.0% 3.0% 3.0%
Discount rate 21 3.0% 3.0% 3.0%
* (Avg) indicates simulations use values that vary across time; the value reported here is the simple average through age 90
Figure 4
Baseline Model Inputs for all scenarios*
11
75% government share of fall costs (line 19). As shown in the numerical results below and
discussed at greater length in the conclusion, smaller government home mod payment shares
do prove to be cost effective, leading to the positive result in this paper.
In the simulation federal government costs are assumed to increase when falls are reduced
from two avenues: fewer deaths mean that some people live longer, so we need to know per
capita federal healthcare spending (line 13) and life expectancy (line 6); modifications that
occur in the first year of the simulation at the government’s expense are substitutes for self-
financed modifications that would have occurred in subsequent years, so we need to know the
existing rate of home mods (line 15).
Documentation for the sources and thinking behind each of the model inputs is provided in
Appendix A. A printout of the model for the Baseline P3 simulation, along with text describing
out the simulation works, is provided in Appendix B.
Figure 5 reports the Baseline results along with selected sensitivity exercises to some of the key
assumptions. The columns report key simulation summary statistics separately for society (the
Direct Financial Savings Results) and for the federal government (Government Savings Results).
For each of these accounting views the columns include: the year that cumulative savings
finally exceed costs (if it occurs), the cumulative net savings at year 10, and cumulative savings
in the final year of the simulation (year 16 for P3).
The full Baseline simulation is displayed in Figure A2; key summary statistics are bolded in the
top line of Table 5. We see it takes 11 years for society to recover the $878M of intervention
costs. The federal government accounting, which recognizes only 75% of the healthcare savings
and includes other modest incremental costs from the intervention, never breaks even. In year
10, the end of CBO’s time frame, the government is carrying an intervention deficit of $420M;
at the end of the simulation in year 16, the government’s discounted deficit has fallen to
$235M.
There is no need to perform sensitivities to the total population figure (lines 1-3 in Figure 4)
since the effect of that number is simply to scale the entire cost effectiveness calculation. If
move-out or death rates are higher than baseline (line 2 in Figure 5), savings are reduced. If the
cost of the home modification is only $2000 instead of the baseline $4400 (line 3) with no
change in fall reduction effectiveness, savings increase and move the society cross-over point
ahead to year 5; the government reaches break even in year 9. If the home modification is only
half as effective in reducing falls than the baseline’s -40% assumption, costs exceed benefits,
with an only slightly smaller effect if the modification’s fall reduction effectiveness degrades
over 5 years to being only half as effective (for P3 to -20% starting in year 6). If fall costs are
$30,000 rather than the baseline’s $11,500 (line 7), savings are greater. Small changes to the
inflation rate or discount rate (lines 8 and 9) yield modest changes to the savings numbers.

12
The federal government remains in the red for the Baseline and most of these sensitivity
exercises. However, reducing the government’s payments for the modification to 50% (line 10)
it breaks even in year 10; reducing its cost share to 20% (line 11), it breaks even in year 4. Line
14 teaches us that the incremental fed cost increments amount to $160M over the ten-year
period (158=420-262). These various sensitivities show that more accelerated net benefits and
a positive federal result are possible for reasonable alternative input values, particularly with
cost sharing, but there is also a good chance the real world economics can be worse than in the
baseline.
12
Figure 6 provides a table for P2 simulation results and sensitivities. Key changes from the P3
simulation are the fall reduction effect of -20% in P2 versus -40% in P3, and the additional ten-
year length of the simulation that gives the opportunity for greater societal savings to
cumulate. Compared to P3, here the baseline Direct Savings no longer show the home
modifications costs are more than balanced by the healthcare savings from fall reduction
(alone). In general, the pattern of results across the sensitivity exercises is similar to P3, but
with a much more delayed cross-over point. If the costs are shared 50/50, the government
12
It’s useful to see how the widely embraced CAPABLE program would present in this framework. Szanton (2019)
only reports program performance metrics around reduced ADL and IADL difficulties, improved walking, self-care
and less depression. But Ruiz (2017) quantifies the healthcare savings as being $2765 per quarter per person for 2
years. With the program spread out over 2012-2016 (so assume 2014 dollars) we can translate that into $13,184
annual savings in 2020 dollars. The program spending per client was $2825 for all services, including up to $1300
in home modification expenses (one third less than our line 3 figure of $2000). Updated to 2020 that’s $3368.
That’s a hugely worthwhile investment: to pay $3368 and receive at least two years of $13,184 savings.
Figure 5
P3 Results Sensitivity to Alternative Input Variable Assumptions
Sensitivity
Specific Change
Year Discounted
Savings > Costs
Cum Net Savings
@ Year 10 ($Mil)
Cum Net Savings @
Cohort aged 90 ($Mil)
Year Discounted
Savings > Costs
Cum Net Savings
@ Year 10 ($Mil)
Cum Net Savings @
Cohort aged 90 ($Mil)
Baseline 1 11 -56 +242 nev er -420 -235
House Tenure
Increase the mortality/move-out
rate by 5 percentage points
2 never -208 -56 never -506 -412
Decrease to $2000 3 5 +423 +721 9 +59 +244
Increase to $10,000 4 never -1174 -876 never -1537 -1353
Decrease fall reduction from -40%
to -20%
5 never -467 -318 never -649 -556
Decrease fall reduction
effectiveness to 50% in year 5
6 never -366 -218 never -594 -502
Increase nonfatal fall cost from
$11,499 to $30,000
7 4 +1234 +2001 6 +492 +1008
Inflation=3%/Discount rate=6% 8 14 -142 +68 never -481 -358
Inflation=6%/Discount rate=3% 9 10 +73 +507 never -347 -77
Reduce Fed HM cost share from
100% to 50%
10 10 +19 +203
Reduce Fed HM cost share from
100% to 20%
11 4 +283 +467
Increase Fed cost share from 75%
to 100%
12 never -255 -5
Reduce Fed Medical cost share
from 75% to 58%
13 never -532 -392
Fed Cost Increments
Zero out Fed increments (R,S) 14 never -262 -38
Fed Cost Sharing
Direct Financial Savings Results
Government Savings Results
Home mod expense
Fall Reduction
Inflation/Discounting

13
savings turn positive now after 23 years rather than the 10 years shown in Figure 5. When the
federal government shares in only 20% of the costs, the government gets its investment back in
8 years, within CBO’s 10-year time horizon.
Results for the P1 simulation are not reported. Using the model as described earlier, there is no
fall reduction savings for the first 15 years until the homeowner turns 65. That eliminates the
prospect for finding any savings to the federal government within the first 10 years.
It’s not only about fall reduction
In the discussion so far the dollar savings from home modifications have come exclusively from
reducing falls that precipitate high healthcare expenses. But C&B identify disciplined studies
that document other less tightly quantified benefits that include improvements in physical and
mental well-being, self-care and independence, and caregiving. A literature survey from the UK
concludes, ‘there are already findings that the provision of housing adaptations and equipment
for disabled people produce savings to health and social care budgets’ (Heywood, 2007, page
9).
Changes to the built environment provide many other advantages to residents that go beyond
fall mitigation and can be measured, but just not so easily in dollars and cents. Findings in the
literature include improving independence and slowing the rate of functional decline generally
(Mann, 1999) and for dementia patients (Gitlan, 2001) and for those with developmental
disabilities (Hammel, 2002) and for those with early-onset disability (Wilson, 2009). Petersson
Figure 6
P2 Results Sensitivity to Alternative Input Variable Assumptions
Sensitivity
Specific Change
Year Discounted
Savings > Costs
Cum Net S avings
@ Year 10 ($Mil)
Cum Net S avings @
Cohort aged 90 ($Mil)
Year Discounted
Savings > Costs
Cum Net S avings
@ Year 10 ($Mil)
Cum Net S avings @
Cohort aged 90 ($Mil)
Baseline 1 nev er -3441 -329 nev er -4912 -3043
House Tenure
Increase the mortality/move-out
rate by 5 percentage points
2 never -4045 -2695 never -5236 -4434
Decrease to $2000 3 10 +148 +3259 20 -1323 +545
Increase to $10,000 4 never -11814 -8702 never -13285 -11416
Decrease fall reduction from -40%
to -20%
5 never -5010 -3454 never -5745 -4811
Decrease fall reduction
effectiveness to 50% in year 5
6 never -4667 -3112 never -5567 -4632
Increase nonfatal fall cost from
$11,499 to $30,000
7 8 +1512 +9549 13 -1341 +4079
Inflation=3%/Discount rate=6% 8 never -3794 -1819 never -5167 -4117
Inflation=6%/Discount rate=3% 9 18 -2915 +2210 never -4630 -1534
Reduce Fed HM cost share from
100% to 50%
10 23 -1623 +246
Reduce Fed HM cost share from
100% to 20%
11 8 +351 +2220
Increase Fed cost share from 75%
to 100%
12 never -4326 -1804
Reduce Fed Medical cost share
from 75% to 58%
13 never -5311 -3885
Fed Cost Increments
Zero out Fed increments (R,S) 14 never -4225 -1891
Fed Cost Sharing
Direct Financial Savings Results
Government Savings Results
Home mod expense
Fall Reduction
Inflation/Discounting

14
(2008) finds no improvement in independence but observes reduced difficulties and greater
safety when performing ADLs. Gitlin (1999) finds greater safety from the installation of
bathroom equipment.
Home modifications can bring reduced dependence on caregivers along with greater safety
(Carnemolla, 2011). A (self-reported) survey of 157 recipients of (Australian) government-
subsidized home modifications with a mean age of 72 years found meaningful reductions in
formal (-16%) and informal (-42%) caregiver hours, (Carnemolla, 2019). The results of Anderson
(2013) are broadly consistent, finding assistive technology, which in that paper includes bath
and toilet rails, to be complements to formal caregiving and substitutes for informal caregiving.
Modest home remodeling expenditures – that may include property maintenance as well as
accessibility improvements - can be valuable for keeping low-income elderly safe and living in
their community rather than forcing them into congregate care facilities and increasing costs to
Medicaid. Relying on a resident’s resourcefulness and existing network of home services for
even a handful of months that delays a move to congregate care can make renovations cost-
effective. Eriksen (2015) finds that accessibility features lower move-out rates leading to a 10%
reduction in nursing home stays during their 2-year observation window. Tinetti (1997) draws a
direct link from serious falls to increased likelihood of moving to a skilled nursing facility. Hwang
(2011) finds that modifications extend the time people age in place in their home, while
Newman (1990) finds the opposite, that they do not reduce the likelihood of
institutionalization.
13
The City of Chicago’s HomeMod Program has reduced the cost of personal
care services and emergency transportation for its participants by roughly $7000, however its
service population is low-income individuals with disabilities under age 60 (Cowan, 2020). A
study for the state of Minnesota providing a cost comparison of home-based living versus
facility-based living identifies a monthly cost difference of $1000 (assisted living) to $4000
(skilled nursing); their estimate of the average renovation expenses needed for their population
was $15,749 (Warren, 2016). Genworth reports annually on the ‘Cost of Care’ across service
providers. Their numbers for 2020 range from homemaker services for someone remaining in
their home (44 hours weekly) at a monthly cost of $4500 to a private room at a nursing facility
at a cost of $8800.
There may also be a benefit from anticipating a potential future need that is not strictly
prevention. Homes that are made accessible to those with disabilities can make it possible for
individuals who require rehabilitative services to return to their home after a hospital stay
rather than be forced to relocate to an institutional setting to remain safe. To our knowledge,
no studies have examined that potential benefit, which is only recently becoming a true option
as home-services and insurance reimbursement allows. Importantly, prepared homes also
support the visitability of family or social acquaintances who require these accommodations.
13
Safran-Norton (2010) identifies a more complex scenario, with couple household transitions unaffected by home
modifications, while single household transitions are reduced by exterior improvements while an increase is
correlated with interior improvements.

15
These comments should not be construed to suggest home modifications are an alternative to
the services of occupational therapists. One would hope that any healthcare situation with an
identified need for OT services is already receiving them. Rather as laid out in Figure 3, here
the emphasis is on prevention before there is an identified need. Should a need then occur, the
presence of already installed accessibility features or government subsidies that facilitate their
timely installation become a tool for successful OT results.
All of these study results and community programs represent an acknowledgement that value
accrues to residents and communities from upgrading their housing stock with accessibility
features. Therefore, the federal government needn’t be the only source of funding, and
perhaps even shouldn’t be.
The Model not Taken
An alternative to the simple modeling approach taken here would be to use a ‘markov macro-
simulation model’. There, as is done here, a starting population transitions through a sequence
of various events leading to differing outcomes and costs until death or a terminal point.
Knowledge of state transition heterogeneity across sub-populations can generate much more
nuanced results than reached here.
Pega (2016) uses this technique to address a very similar question to ours: ‘to determine the
health gain, cost-utility and health equity impacts from home safety assessment and
modification (HSAM) for reducing injurious falls in older people.’ They analyze the cost-
effectiveness of a HSAM program in place for 65+ year-olds in New Zealand that pairs an OT
assessment with home modifications, including total intervention costs in 2011 of only
US$169(!). The model input assumption of the fall reduction magnitude from the intervention
is -19%, drawn from Gillespie (2012).
Pega’s broad conclusions are strikingly similar to ours here: lifetime dollars saved do not
cumulate to exceed upfront costs; concentrating efforts on higher risk populations (either those
older or those with a history of falls – roughly our P3 versus P2) reduces the cost-effectiveness
gap but doesn’t flip the results to net savings. In addition to dollars they measure savings in
terms of ‘quality adjusted life years’ (QALY), a metric that has been in use since the 1960s and
embraced by the WHO and in many countries.
14
They find significant gains in QALYs and a very
favorable incremental cost effectiveness ratio (ICER) of $6000(US) per QALY, far below the
standard threshold of $50,000 per QALY. They point out that concentrating efforts on higher
risk populations does create better ICERs and could well be the prudent starting point for policy
14
The British National Health Service uses QALY metrics to resolve competing demands for treatment within its
limited financial resources. QALY offers a systematic process for combining morbidity (quality of life) and mortality
(length of life) into a single index that can be used to evaluate the relative benefits of qualitatively different
treatments. Despite its perhaps dubious theoretical underpinnings, it has been embraced through its introduction
of rigor and sheer convenience MacKillop (2018). However, the commonly cited threshold of $50,000/QALY
warrants review (Marseille (2014), Neumann (2014)).

16
initiatives, but that total QALYs saved by society will be lower than with a broad-based (i.e. P2
type) approach.
15
Limitations
A consistent theme from the many SLRs that consolidate results from the wide range of fall
mitigation programs is concern over their small samples and hence limited ‘power’ (the ability
to reject a false hypothesis). That naturally leads to efforts like Gillespie (2012) to commingle
data across even heterogeneous studies.
We acknowledge that challenge, which is one of the reasons we have emphasized the careful
study by Eriksen (2015). A presumption that the placement of accessibility features in the
home, even without the guidance of an occupational therapist, will bring a meaningful
reduction in falls is central to achieving the cost-effectiveness of government support. While
the breadth of multifactorial study results are consistent with the 20%/40% reductions used
here, only the Eriksen study supports the results for a modification-only intervention. And of
course, the Ericksen paper itself identifies its own potential limitations.
16
There are abundant reasons one could question the strength of our result and hence the
implications of this study: it is possible that those individuals at greater risk (e.g. already fell)
might be more proactive at mitigating their own risks, limiting the nascent fall savings from the
remainder incented to build in accessibility features (sensitivity #5); we assume no depreciation
in the effectiveness of the intervention through the home tenure, which may be too aggressive
as studies frequently report people reverting to former behaviors (sensitivity #6). Our analysis
assumes there is no correlation between individual fall frequency and remediation costs, even
though in the real world the distribution of population falls is skewed towards multiple falls of a
more intensely at-risk population, making it likely that these multiple-fallers will endure quicker
mortality or institutionalization and thus may not generate savings for as many years as
assumed in the model (sensitivity #2). To simplify the simulations we have assumed all of the
modification benefits occur immediately, when in practice it could take many months to
complete all modifications, changing costs little but shaving the fall-reduction benefits. Each of
15
Olij (2018) is an SLR that reviews the effectiveness of a cross section of 31 fall mitigation programs (exercise,
home assessment, medication adjustment, multifactorial, other) through the lens of their reported ICERs, finding
‘investing in fall prevention programs for adults aged 60 and older is cost-effective, particularly home assessment
for community-dwelling older adults… programs were found to be more cost-effective as the age of participants
increases.’ Frick (2010) finds home modification programs that include OT and PT services to be the ‘best value’
across alternative hip-fracture reduction programs, costing $14,794/QALY. Jutkowitz (2012) calculates ICER
relative to a straightforward measure of ‘life years saved’ (LYS) by tracking mortality 2 years after the ABLE (the
pre-CAPABLE) program intervention in 2003. They find a $13-15,000 cost per LYS. A back-of-the-envelope
calculation at the end of Keall (2015) finds a favorable ICER relative to a measure of ‘disability adjusted life-years’
(DALYs) from their HSAM program.
16
Turner (2011) reads many of the same papers discussed here and comes to the, to us inexplicable, conclusion
that ‘there is very little high-grade evidence that interventions to modify the home physical environment affect the
likelihood of sustaining an injury in the home.’

17
these cautions warrants a close look, even as we believe the core message here is sound and
should not be subject to death-by-a-thousand-cuts.
Conclusion and Policy Implications
This paper has not produced a new result that overturns the tepid ‘C’ rating by the US
Preventive Services Task Force on the preventative benefits of home modifications.
17
But
Stevens (2005) gets right to the point that ‘falls and fall-related injuries represent an enormous
burden to individuals, society, and to our health care system. Because the U.S. population is
aging, this problem will increase unless we take preventive action. We need to refine, promote,
and implement effective interventions.’ Kochera (2002) goes further to observe that
‘approaching programs from a cost perspective focuses on what can be easily measured or
estimated and does not include other hard to quantify, but arguably more important, factors
such as improved quality of life and peace of mind for older persons and their families. In
addition, this type of approach does not factor in the non-health care costs that older persons
and their families save (such as lost time from work) as a result of fewer falls.’ More than 15
years later, this paper provides a path to moving more aggressively from research to modifying
behaviors and practice, as noted in Noonan (2011).
The surest way to provide homeowners with a nudge to stimulate them to modify their home
to anticipate future needs and prevent falls is to give them a financial incentive. The model
simulation here demonstrates that the federal government can do that and get a positive
return when it shares the up-front expense. For the P3 population, even paying up to 50% of
the home modification costs would allow the government to recoup all of its upfront
investment within CBO’s 10-year methodology window. For the P2 population, the federal
government reaches a cross-over point in year 8 with a 20% cost sharing. That could be
accomplished by allowing qualified home modification expenditures to be deductible against
income taxes.
The model simulation for the P1 population in this paper might appear to be guaranteed to fail
CBO’s effectiveness criteria since we seek to change homeowner behavior when they are in
their 50s while the benefits don’t start accruing until after the homeowner is 65 years old and
17
The US Preventive Services Task Force (USPSTF) performs the important role of constantly sifting through
medical research to provide an official government imprimatur on when the research is convincing enough to
demonstrate efficacy of proposed cures or preventive interventions. Their highest level of endorsement is an ‘A’
rating that there is a high certainty of benefit. Medical insurance offerings are required to cover expenses related
to ‘A’ interventions as well as those with a ‘B’ rating of moderate to substantial benefit. USPSTF (2018), consistent
with its earlier 2012 study, found that ‘multifactorial interventions’ which might include home modifications as a
component of a suite of activities warrant a ‘C’ rating, using language stating “The USPSTF recommends selectively
offering or providing this service to individual patients based on professional judgment and patient preferences.
There is at least moderate certainty that the net benefit is small.”

18
covered by Medicare/Medicaid. But allowing an exemption from the current 10% penalty for
early withdrawal of funds in an IRA/401k investment pool would not cost the federal
government revenue while achieving the important goal of providing a financial ‘nudge’ at
exactly the time the homeowner is going through a home renovation.
18
As stated in Powell
(2017), ‘there is good evidence that people can be put off installing adaptation until they reach
a point of crisis, in part because they do not wish to change or ‘medicalise’ their home.’ A
nudge at the moment when remodeling work is already being performed could start to change
that mindset.
When it comes to program design, requiring the insurance and client beneficiaries to have
some skin in the game of home renovations is likely a good idea to limit waste and fraud. The
precise details of how to craft a tax credit/exemption/deduction that achieves the desired
purposes are not the focus here and can be left to others.
19
Experience of one retailer suggests
that a 20% discount can be sufficient to pivot consumer behavior (Lieber, 2020)
The societal need for safely aging in place is already upon us, with education and training
promoted by the Administration for Community Living and other organizations. It is our hope
that the introduction of government subsidies for home accessibility improvements, prompted
by the disciplined support given here, can similarly catalyze demand and supply in the home
remodeling industry to address this current need.
18
There are understandable policy concerns regarding the wisdom of allowing early withdrawals from retirement
savings (Bernstein, 2021). We would point out that home improvements are a way to transform personal financial
capital into physical capital (their home) that has the potential to create a tremendous return during retirement.
Of course, as with any investment, there is no certainty regarding the magnitude of that return.
19
The legislative objectives here fit well within the mainstream of bipartisan proposals currently circulating on
Capitol Hill, such as the Choose Home Care Act of 2021 S.2562 and the Americans Giving Care to Elders (AGE) Act
S.234/HR.3689.
19
Appendix A – Model Inputs
Population
The P3 population is the number of owner-occupied households where at least one individual
turns 75 years old in 2020 and where this individual has multiple chronic conditions with
limitations of at least one ADL and one IADL. This is derived from Joint Center household
estimates (Spader, 2019). Their base estimate of households headed by a 70-74 year old in
2018 is 6.878 million. Assuming an even distribution by age and shaving that figure by two
years of mortality (3%/year) and move-outs (1.7%/year) yields 1,250,747 million households.
Using the same methodology for P2, 65 year-old households (with 1.3% mortality and 0.8%
move-outs) yields 1,759,036. Using the same methodology for P1, 50 year-old households
(with 0.4% mortality and 0.8% move-outs) yields 1,491,868.
Reality check: These figures are reasonably close to the 2019 AHS report of owner-occupied
households if we take one-tenth of the 10-year spans of 65-74 year households (14,696,000),
55-64 year households (18,602,000) and 45-54 year households (15,135,000).
Data from the 2014 University of Michigan Health and Retirement Study finds that 28% of 65-
79 headed households have a mobility disability, and if self-care disabilities are included the
total may be higher (Joint Center, 2016). Reality check: the 2019 AHS reports a variety of
disability categories; assuming the ‘not reported’ numbers distribute proportionately, 34% of
65-74 householder residences are ‘with a disabled person.’
Some of the properties occupied by these households will already be equipped with
accessibility features, so are not in need of further improvements. This will reduce the ‘eligible
population’ of individuals or structures for P3. The 2019 AHS finds that of the 75+ households
identified as ‘disabled’, that 43% (=(806+2320)/7246) rated their home as meeting their
accessibility needs with a 4 or 5 out of a 5 point scale. That suggests that the total number of
properties that are prospects for home modifications may be only 57% of the population with a
disability. Among all households 65 to 74 the percentage with a 4 or 5 is 15%, and for
households 55 to 64 the percentage is 9%.
Reality Check: Liu (2009) find that 38% of households with 70+ year olds had some accessibility
features in 1995.
Moves and Deaths
Each year some of the community-living adults in owner-occupied housing will move out of
their homes for a variety of reasons that can include lifestyle, moving to be close to kids, to
move in with kids, or to a congregate care facility. Any of these moves eliminates the fall-
reduction savings of installed accessibility features. Munnell (2020) uses the University of

20
Michigan’s Health and Retirement Survey (HRS) to segment the population into cohorts they
call: never movers, stable movers (move once around retirement), frequent movers (lifestyle)
and late movers (likely healthcare motivated) whose shares differ between their 50-54 age
cohort, their 70-74 age cohort and their synthetic cohort. In Figure A1 just below we translate
their cohort shares into annual move-out rates for our age 50, 65 and 75 cohorts for three
different age ranges.
Reality check: Safran-Norton (2010) finds much higher transitions in the 1998 and 2000 waves
of the HRS for the 65+ cohort: over that two year period 7.4%(8.7%) of couples(singles) moved
primary residence, while 1%(4%) moved into nursing homes and 6.7%(9.5%) died.
In addition to move-outs, we need to know the mortality rate and expected longevity for
individuals at each age of life. This information is provided by the Census Bureau for 2017
(Medina, 2020). Our values are a simple average of the male and female rates; no adjustment
was made for the underlying data being three years prior to 2020.
Fall Rates
According to a CDC phone survey in 2014, (Bergen, 2016) 28.7% of community-dwelling adults
65 years or older reported falling, of which 37.5% needed medical treatment or restricted their
activity for a day or longer. The survey results are broken out by age ranges of 65-74, 75-84 and
85+, yielding 26.7%, 29.8% and 36.5% for individual fall rates, and of those falls, 36.3%, 36.6%
and 37.9% for serious falls, respectively. Taken together the average figures yield a roughly
Age 50-54 Age 70-74 Synthetic Age 50 Age 65 Age 75
Never Movers 63% 75% 53%
Stable Movers 19% 7% 17% 17%/40yrs 7%/25yrs 7%/15yrs
Frequent Movers 18% 11% 14% 14%/40yrs 14%/25yrs 11%/15yrs
Late Movers 8% 16% 16%/15yrs 16%/15yrs 8%/15yrs
Derived Annual Move out rates used in this paper
Ages 50-64 0.0078
Ages 65-74 0.0078 0.0084
Ages 75+ 0.0184 0.0191 0.0173
Source: Munnell (2020)
We assume mortality at age 90; age 65 cohort is blend of age 70-74 and synthetic cohort values
Original Paper's Cohorts
Translation to Our Cohorts
Figure A1
Derivation of Annual Move-out Rates for Simulation
21
11% (=0.287*0.375) ‘serious’ fall rate; in the model we use the age-specific rates. In absolute
numbers, for 65+ year olds, the CDC reports 29 million falls, 7.0 million fall injuries, 2.8 million
emergency room visits, 800,000 hospital stays and 27,000 deaths. The CDC reports a 10.5 bps
annual mortality rate from falls over 2008-2014 for ages 75+, 1.4 bps for ages 65-74 and 0.5 bps
for 50-59.
Reality Check: Kochera (2002) finds a 5% serious fall rate that requires emergency room
services. Todd (2020) finds a 2.1% rate for Philadelphians 65+ year olds being admitted to
hospitalization from falls in 2018; 75+ year olds had a higher 4.5% fall-driven admit rate. Todd
also finds 3% mortality from serious falls, yielding a 6 bps rate of death for 65+ Philadelphians.
Fall Costs
The source of fall costs is Burns (2016) which bases non-fatal costs on 1998-99 data updated
with a healthcare inflator. Their 2012 cost estimate for fatal falls is $25,487 and for non-fatal
falls is $9463. The cumulative PCE healthcare deflator (what they use and is consistent with the
US BEA’s recommendation) increase from 2012 to 2020 is 21.52% yielding 2020 costs of
$30,972 and $11,499, respectively.
Reality Check: The Senate Committee on Aging (Collins, 2019) reports a $30,000 cost per fall-
generated hospital stay, citing Burn’s $30,550 figure for 2012 hospital costs. Data for
Philadelphia from Todd (2020) reports a higher $65,000 average cost for a median four-day
hospital stay.
Bottomline Reality Check. The Senate report estimates the annual cost of falls for 65+ year-olds
is $50 billion, taken from Florence’s (2016) number for 2015. Increasing that figure by the
17.9% increase in the PCE and 16.8% population increase from 2015 to 2020 gives $69 billion,
close to what we get from a 55.7 million 65+ population in 2020, times 11% fall rate times a
$11,499 cost per fall yielding $71 billion.
Home Improvement
Each household starts with a different physical layout while each resident will have their own
unique needs, making it evident than no single dollar figure can capture what will be needed to
make any specific home ‘accessible.’ And what is needed for any individual will evolve over
time. Home modification expenditure budgets vary considerably across the papers cited with
published results: Jutkowitz (2012) gives the average modification spending in the ABLE
program to be $439 in $2010. Szanton (2019) gives the average modification spending in the
CAPABLE program of $1222; Plautz (1996) cites an average hard cost of $92.80 and $50-100 for
labor; Keall (2015) cites a $450 (US) figure; Eriksen (2015) cites a $1700 figure (in $2000) spent
over a two-year period on home modifications from their longitudinal data source. Heywood
(2007) cites an average cost of a disabled facilities grant as being £6000 that typically includes a
stairlift and a level access shower.
22
Community programs that provide home modifications to low-income residents have a much
higher dollar threshold than these academic studies: the DC Safe at Home program has a cap of
$6000 and spent an average of $3700 per client on home modifications in early 2020 (private
correspondence); the Federal Home Loan Bank (FHLB) of Indianapolis’ Accessibility Modification
Program offers grants up to $12,000 (and can include regular home repairs); the Carol M.
Peterson Housing Fund at the FHLB of Cincinnati offers grants up to $7500. The City of
Chicago’s HomeMod Program spends between $12,200 and $15,150 per participant, though
they are serving those with a disability under age 60 and often install vertical power lifts
(Cowan, 2020). In its study for the State of Minnesota, Wilder Research estimated the average
cost of safety home improvement needs of low-income older adult homeowners at $6989 per
household (Warren, 2016, p54).
The JCHS (2021) reports the average expenditure on ‘discretionary’ home remodeling was
$13,302. The HomeAdvisor website says that the average grant for an accessibility remodel will
be $4350 in 2021.
We adopt HomeAdvisor’s $4400 figure, perhaps erring on the high side. Some of the programs
written about benefit from below-market labor costs (Plautz uses VISTA workers; CAPABLE uses
Americorps). While the hard costs for a few grab bars and a raised toilet seat can run only a
few hundred dollars, too small a dollar amount for a federal tax deduction program can make it
too unattractive and hence unused.
Federal government healthcare costs
Kochera (2002) estimates that 75% of the $9359 total direct cost of falls leading to an
emergency room visit for 65+ year olds in 2000 is covered by the federal government. An
alternative estimate can come from CMS which reports annually on national health
expenditures. Their most recent breakdown by recipient age is for 2014, and shows that in
total, Medicare covered 52% of spending for 65+ year olds and Medicaid another 10%. Figures
from Kochera (2002) show the federal share of Medicaid spending to be 56%, suggesting a
perhaps total 58% for the federal share of healthcare spending for 65+ year olds
(0.576=0.52+0.56*0.10). Given the striking consistency of the $9359 and Burns (2016) $9463
figures, we will use the 75% federal government share in our baseline and run a sensitivity with
the 58% figure.
Additional Costs From Reduced Falls
The CBO methodology seeks to derive net government savings compared to current policies.
We include two calculations that reduce the net government savings versus direct savings: an
estimate of how much reduced falls leading to mortality can increase government medical
insurance costs, and we haircut the government savings from subsidized modifications that
simply replace future self-initiated home modifications.
23
It is too complicated to consider whether there are higher medical costs for people who now
don’t fall but who previously fell and survived. But we can estimate how much healthcare
those now non-dead people might consume on average over the rest of their lives. CMS puts
the per-person healthcare spending in 2014 for individuals 65+ at $19,098. The healthcare PCE
indicates cumulative inflation was 19.2% to 2020, bringing that to $22,765 in 2020. Assuming
75% of that is federal expense yields an average annual M/M cost of $17,074. For each person
who doesn’t die, we multiply that annual cost by the remaining years of life expectancy. (We
use the inflated nominal dollar figure from the year life is saved for all of the subsequent years.)
Reality check. CMS reports the Medicaid spending per enrollee in 2018 for individuals 65+ of
$18,272 for low level data useability (close to the $18,583 average of the medians for high,
moderate and low data useability). Medicare spending per enrollee in 2019 was $10,536. The
healthcare PCE shows a 5.1% increase from 2018 and 2.6% from 2019 to bring both Medicaid
($19,204) and Medicare ($10,811) numbers to 2020 and a 43/57 split (to match 2019
expenditures) yields an estimate of $14,420, which is 84% of the number above. Close enough.
There is another source of increased costs to the government from their providing widespread
home modifications. Many individuals every year make their own home improvements without
the benefit of government subsidies, with the resulting healthcare savings already built into
existing fall and cost statistics. For these people, a government intervention is effectively
paying for the modifications (and getting the medical savings) ‘earlier’ in time. The healthcare
savings the federal government is currently receiving ‘free’ but would now start paying for is an
incremental cost from the federal government’s perspective. To calculate this cost to the
government we turn to the 2019 AHS, which asked: how many owner-occupants planned to
make accessibility improvements over the next two years? And we accept the answer at face
value. For 75+ year olds with disabilities that figure is 8.6% yielding an annual rate of 4.3%. For
all 65+ year olds the annual figure is 2.9%. Therefore either 4.3% or 2.9% of the nonfatal falls
‘savings’ are not net-new savings but would have already happened in the baseline each year,
so these need to be removed from the estimate of annual government savings.
Appendix B – Baseline P3 Model Simulation
How the model plays out in each year for the Baseline P3 simulation is shown in Figure A2. The
starting population is 199,619 (line C) households that reflect the product of the numbers in
lines 1-3 (of Figure 4). For simplicity, all of these households are assumed to instantaneously
receive a home modification on the first day of the calendar year they turn 75, which is also the
first day of the simulation. Falls occur at rates in lines 9 and 10, which using costs in lines 11
and 12 create total costs in lines E and F; The Line 16 percent of falls don’t occur creating
savings in line G, which are cumulated in line H. Households are decremented annually by
move-outs and deaths (lines K and L).
24
The intervention hard-cost is line M. Savings (line G) are increased by inflation (line 20) and
decreased by the discount rate (line 21) to create discounted savings in lines N and O. Line P is
line O plus line M.
The federal government’s costs include its share of the modification costs (line Q), the
increased Medicaid/Medicare cost of fewer deaths in lines I and J yields line R and an estimate
of the savings individuals would have gained from future self-modifications that have been pre-
empted by the government’s action at age 75 (line S). That yields the annual and cumulative
increase in nominal federal costs (lines T and U) and discounted costs (lines V and W). Netting
costs versus savings (lines X and Y) yields net federal costs (line Z).
In the baseline scenario where cost inflation exactly matches the discount rate, it takes 11 years
for society to recover the $878M of intervention costs. The cells that show this result are
highlighted in orange. In year 10, the end of CBO’s time frame, the government is carrying an
intervention deficit of $420M; at the end of the simulation in year 16 the government’s
discounted deficit falls to $235M. The cells that show this result are highlighted in green.

25
Model
Year A 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16
Age B Age 75 Age 76 Age 77 Age 78 Age 79 Age 80 Age 81 Age 82 Age 83 Age 84 Age 85 Age 86 Age 87 Age 88 Age 89 Age 90
Population
At risk C 199,619 190,118 180,448 170,622 160,662 150,584 140,376 130,046 119,647 109,245 98,903 88,681 78,642 68,866 59,446 50,494
Percent remaining D 95% 90% 85% 80% 75% 70% 65% 60% 55% 50% 44% 39% 34% 30% 25%
Risk events
Cost of serious falls (net of HM) E (154,721)$ (151,777)$ (148,379)$ (144,508)$ (140,155)$ (135,304)$ (129,916)$ (123,966)$ (117,475)$ (110,479)$ (130,666)$ (120,676)$ (110,226)$ (99,418)$ (88,394)$ (77,336)$
Cost of fatal falls (net of HM) F (4,012)$ (3,936)$ (3,847)$ (3,747)$ (3,634)$ (3,508)$ (3,369)$ (3,214)$ (3,046)$ (2,865)$ (2,671)$ (2,467)$ (2,253)$ (2,032)$ (1,807)$ (1,581)$
Net Costs saved because of home mod G 105,822$ 103,808$ 101,484$ 98,837$ 95,859$ 92,541$ 88,856$ 84,787$ 80,347$ 75,563$ 88,892$ 82,095$ 74,986$ 67,634$ 60,134$ 52,611$
Cumulative Nominal savings H 105,822$ 209,630$ 311,114$ 409,951$ 505,810$ 598,351$ 687,208$ 771,995$ 852,342$ 927,905$ 1,016,796$ 1,098,892$ 1,173,878$ 1,241,512$ 1,301,646$ 1,354,257$
Fewer deaths b/c of fall reduction I 84 80 76 72 67 63 59 55 50 46 42 37 33 29 25 21
Incr. cost from longer lives J (23,650)$ (21,946)$ (20,276)$ (18,627)$ (17,016)$ (15,438)$ (13,907)$ (12,428)$ (11,023)$ (9,672)$ (8,404)$ (7,223)$ (6,123)$ (5,119)$ (4,219)$ (3,420)$
Move outs K 3,453 3,289 3,122 2,952 2,779 2,605 2,429 2,250 2,070 1,890 1,711 1,534 1,361 1,191 1,028 874
Deaths L 6,048 6,381 6,704 7,008 7,299 7,603 7,901 8,150 8,332 8,451 8,511 8,505 8,416 8,228 7,923 7,494
Financial Results
intervention cost M (878,325)$
Discounted Home Mod Savings N 105,822$ 100,785$ 95,659$ 90,450$ 85,170$ 79,827$ 74,416$ 68,940$ 63,427$ 57,913$ 66,144$ 59,308$ 52,594$ 46,055$ 39,756$ 33,769$
Cumulative Discted Savings O 105,822$ 206,606$ 302,265$ 392,715$ 477,884$ 557,711$ 632,127$ 701,067$ 764,493$ 822,406$ 888,550$ 947,857$ 1,000,451$ 1,046,507$ 1,086,262$ 1,120,031$
Cumulative Net Fin S avings P (772,503)$ (671,718)$ (576,060)$ (485,610)$ (400,440)$ (320,613)$ (246,198)$ (177,258)$ (113,831)$ (55,919)$ 10,225$ 69,533$ 122,127$ 168,182$ 207,938$ 241,707$
Federal Government
Govt Modification Costs Q (878,325)$
Fed Incr. cost from longer lives R (17,737)$ (16,460)$ (15,207)$ (13,971)$ (12,762)$ (11,579)$ (10,430)$ (9,321)$ (8,267)$ (7,254)$ (6,303)$ (5,417)$ (4,592)$ (3,839)$ (3,165)$ (2,565)$
Fed Incr. Baseline savings from self mod S (4,550)$ (4,334)$ (4,113)$ (3,889)$ (3,662)$ (3,433)$ (3,200)$ (2,964)$ (2,727)$ (2,490)$ (2,844)$ (2,550)$ (2,262)$ (1,980)$ (1,709)$ (1,452)$
Annual Incr. Nominal Fed Costs T (900,612)$ (20,793)$ (19,321)$ (17,860)$ (16,424)$ (15,011)$ (13,630)$ (12,285)$ (10,995)$ (9,744)$ (9,147)$ (7,968)$ (6,854)$ (5,820)$ (4,874)$ (4,017)$
Cumulative Nominal Fed Costs U (900,612)$ (921,405)$ (940,726)$ (958,586)$ (975,010)$ (990,021)$ (1,003,651)$ (1,015,936)$ (1,026,931)$ (1,036,675)$ (1,045,822)$ (1,053,790)$ (1,060,643)$ (1,066,463)$ (1,071,337)$ (1,075,355)$
Annual Discted Fed Costs V (900,612)$ (20,188)$ (18,212)$ (16,344)$ (14,592)$ (12,949)$ (11,415)$ (9,989)$ (8,679)$ (7,468)$ (6,806)$ (5,756)$ (4,807)$ (3,963)$ (3,222)$ (2,579)$
Cumulative Discted Fed Costs W (900,612)$ (920,800)$ (939,011)$ (955,356)$ (969,948)$ (982,897)$ (994,312)$ (1,004,301)$ (1,012,980)$ (1,020,448)$ (1,027,254)$ (1,033,010)$ (1,037,817)$ (1,041,780)$ (1,045,003)$ (1,047,581)$
Nominal Govt savings X 79,366$ 77,856$ 76,113$ 74,128$ 71,894$ 69,406$ 66,642$ 63,590$ 60,260$ 56,672$ 66,669$ 61,572$ 56,240$ 50,725$ 45,101$ 39,458$
Cumulative G ovt Nominal S avings Y 79,366$ 154,955$ 226,699$ 294,536$ 358,413$ 418,283$ 474,095$ 525,800$ 573,370$ 616,804$ 666,412$ 710,893$ 750,338$ 784,880$ 814,697$ 840,024$
Cumulative Net Fed Savings Z (821,246)$ (766,451)$ (714,027)$ (664,050)$ (616,597)$ (571,737)$ (529,556)$ (490,136)$ (453,561)$ (419,871)$ (379,410)$ (342,897)$ (310,305)$ (281,583)$ (256,641)$ (235,331)$
Figure A2
Baseline Model Simulation of P3 Cohort

26
References
1. AARP (2012) United States of Aging Survey,
https://www.aarp.org/content/dam/aarp/livable-communities/old-learn/research/the-
united-states-of-aging-survey-2012-aarp.pdf
2. Abrams A (2021) COVID-19 Exposed the Faults in America’s Elder Care System. This is
our Best Shot to Fix Them, TIME, June 15, 2021.
file:///Users/jessemabraham/Zotero/storage/UE6UHRDG/elder-care-after-covid-
19.html
3. Academy Health (2013) The Economics of Prevention, Research Insights.
https://academyhealth.org/sites/default/files/ah_ri_2013_economics_preventionedit2.
pdf
4. Agree EM, Freedman VA, Cornman JC, Wolf DA, Marcotte, JE (2005) Reconsidering
substitution in long-term care: when does assistive technology take the place of
personal care? J Gerontol B Psychol Sci Soc Sci, September, 2005, 60(5) ppS272-S280.
https://doi.org/10.1093/geronb/60.5.s272
5. Ahn M, Hegde A (2011) Perceived aspects of home environment and home
modifications by older people living in rural areas, J Hous Elder, 25(1) pp18-30.
https://doi.org/10.1080/02763893.2011.545735
6. Anderson WL, Wiener JM (2013) The impact of assistive technologies on formal and
informal home care, Gerontologist, June, 2015, 55(3). pp422-433.
https://doi.org/10.1093/geront/gnt165
7. AP-NORC (2021) Long-Term Care in America: Americans want to Age at Home,
https://www.longtermcarepoll.org/project/long-term-care-in-america-americans-want-
to-age-at-home/
8. Bergen G, Stevens MR, Burns ER (2014). Falls and Fall Injuries Among Adults Aged ≥65
Years — United States, 2014. MMWR Morb Mortal Wkly Rep 2016;65:993–998.
http://dx.doi.org/10.15585/mmwr.mm6537a2external icon
9. Bernstein D (2021) Pre-retirement use of 401(k) funds, Business Economics, 56 pp 81-86.
https://doi.org/10.1057/s11369-021-00214-7
10. Bo’sher L, Chan S, Ellen IG, Karfunkel G, Liao HL (2015) Accessibility of America’s Housing
Stock: Analysis of the 2011 American Housing Survey (AHS), Economic Systems Inc. for
US HUD PD&R, March 19, 2015.
https://www.huduser.gov/portal/sites/default/files/pdf/accessibility-america-
housingStock.pdf
11. Burns ER, Stevens JA, Lee R (2016) The direct costs of fatal and non-fatal falls among
older adults – United States, J Safety Res, Sep;58 pp 99-103. 10.1016/j.jsr.2016.05.001
12. Carnemolla P, Bridge C (2011) Home modifications and their impact on waged care
substitution, Report no. 978-0-7334-2893-7: Home Modification Information
Clearinghouse, University of New South Wales, Sydney.
http://www.homemods.info/Download.ashx?File=861ae45c388445cc1a024922a2aa734

27
13. Carnemolla P, Bridge C (2018) A Scoping Review of Home Modification Interventions –
Mapping the Evidence Base. Indoor and Built Environment, online: February 28, 2018.
Published: 2020 29(3), pp 299-310
https://journals.sagepub.com/doi/10.1177/1420326X18761112
14. Carnemolla P, Bridge C (2019) Housing Design and Community Care: How Home
Modifications Reduce Care Needs of Older People and People with Disability. Int J
Environ Res Public Health, 16(11) pp 1951. https://doi.org/10.3390/ijerph16111951
15. Carroll AE (2018) Preventive Care Saves Money? Sorry, It’s Too Good to be True, New
York Times, January 29, 2018.
https://www.nytimes.com/2018/01/29/upshot/preventive-health-care-costs.html
16. Center for Universal Design, (1997) A Blueprint for Action: A Resource for Promoting
Home Modifications, School of Design NC State, http://www.ncsu.edu/ncsu/design/cud
17. Centers for Medicare and Medicaid Services, National Health Expenditure Data,
https://www.cms.gov/research-statistics-data-and-systems/statistics-trends-and-
reports/nationalhealthexpenddata
18. Chase CA, Mann K, Wasek S, Arbesman M. (2012) Systematic Review of the Effect of
Home Modification and Fall Prevention Programs on Falls and the Performance of
Community-Dwelling Older Adults, Am J Occup Ther, 2012; 66: pp284-291.
http://dx.doi.org/10.5014/ajot.2012.005017
19. Clemson L, Cummings RG, Kendig, H, Swann M, Heard R, Taylor K (2004) The
Effectiveness of a Community-Based Program for Reducing the Incidence of Falls in the
Elderly: A Randomized Trial, J Am Geriatric S, September 2004 52(9) pp1487-1494.
10.1111/j.1532-5415.2004.52411.x
20. Clemson L, Mackenzie L, Ballinger C, Close JCT, Cumming RG (2008) Environmental
Interventions to Prevent Falls in Community-Dwelling Older People: A Meta-Analysis of
Randomized Trials, J Aging and Health, December, 2008, 20(8) pp954-971.
https://doi.org/10.1177/0898264308324672
21. Close J, Ellis M, Hooper R, Glucksman E, Jackson S, Swift C (1999) Prevention of falls in
the elderly trial (PROFET): a randomized controlled trial, Lancet, 353(9147) pp93-97.
https://doi.org/10.1016/S0140-6736(98)06119-4
22. Collins SM, Casey RP (2019) Falls Prevention: National, State, and Local Solutions to
Better Support Seniors. Special Committee on Aging United State Senate
https://www.aging.senate.gov/imo/media/doc/SCA_Falls_Report_2019.pdf
23. Congressional Budget Office (2020) How CBO Analyzes Approaches to Improve Health
Through Disease Prevention, https://www.cbo.gov/publication/56345
24. Convergence Center for Policy Resolution (2020) Rethinking Care for Older Adults
https://convergencepolicy.org/wp-content/uploads/2020/12/Rethinking-Care-for-
Older-Adults_12-10-20.pdf
25. Cowan SM, Guzon JE (2020) Assessing Costs and Benefits of Chicago’s CDBG-Funded
HomeMod Program. September, 2020. HUD PD&R.
https://www.huduser.gov/portal//portal/sites/default/files/pdf/Costs-And-Benefits-
HomeMod-Program.pdf

28
26. Crowell JA, Shen X, Sokas R. (2017) Evaluation of the DCOA Safe at Home Program,
prepared for the DC Office on Aging by the Georgetown University School of Nursing
and Health Science, mimeo
27. Cummings RG, Thomas, M, Szonyi G, Salkeld G, O’Neill E, Westbury C, Frampton G.
(1999) Home Visits by an Occupational Therapist for Assessment and Modification of
Environmental Hazards: A Randomized Trial of Falls Prevention, J Am Geriatr Soc, 47(12)
pp1397-1999. https://doi.org/10.1111/j.1532-5415.1999.tb01556.x
28. Cusato M (2016) HomeAdvisor Insight Forum: 2016 Aging in Place Report, October 2016
29. Day L, Fildes B, Gordon I, Fitzharris M, Flamer H, Lord S (2002) Randomised factorial trial
of falls prevention among older people living in their own homes, BMJ, 325(7356):128
https://doi.org/10.1136/bmj.325.7356.128
30. Economist (2020) Who cares? The pandemic shows the urgency of reforming care for
the elderly, Economist International, July 25, 2020.
https://www.economist.com/international/2020/07/25/the-pandemic-shows-the-
urgency-of-reforming-care-for-the-elderly
31. Eriksen MD, Greenhalgh-Stanley N, Engelhardt GV (2015). Home safety, accessibility,
and elderly health: Evidence from falls. Journal of Urban Economics, 87, 14-24.
https://doi.org/10.1016/j.jue.2015.02.003
32. Federal Home Loan Bank of Cincinnati, https://www.fhlbcin.com/housing-
programs/carol-m-peterson-housing-fund/
33. Federal Home Loan Bank of Indianapolis, https://www.fhlbi.com/products-
services/community-investment-and-housing/homeownership-initiatives/accessibility-
modification-program-(amp)
34. Florence CS, Bergen G, Atherly A, Burns E, Stevens J, Drake C (2018) Medical Costs of
Fatal and Nonfatal Falls in Older Adults, J Am Geriatr Soc, 66(4) pp 693-698.
https://doi.org/10.1111/jgs.15304
35. Frick KD, Kung JY, Parrish JM, Narrett MJ (2010) Evaluating the Cost-Effectiveness of Fall
Prevention Programs that Reduce Fall-Related Hip Fractures in Older Adults, J Am
Geriatr Soc, 58(1) pp136-141. https://doi.org/10.1111/j.1532-5415.2009.02575.x
36. Gaydayenko Y, Alexander L (2020) A Solutions-Oriented Partnership Helps Metro Detroit
Elders stay Safe at Home, Generations Journal. https://generations.asaging.org/metro-
detroit-elders-safe-home-aging-place
37. Genworth, Cost of Care Survey. https://www.genworth.com/aging-and-
you/finances/cost-of-care.html
38. Gillespie LD, Robertson MC, Gillespie WJ, Sherrington C, Gates S, Clemson LM, Lamb SE
(2012) Interventions for Preventing Falls in Older People Living in the Community
(Review), The Cochrane Library, 9 https://doi.org/10.1002/14651858.CD007146.pub3
39. Gitlin LN, Miller KS, Boyce A. (1999) Bathroom modifications for frail elderly renters:
outcomes of a community-based program. Technology and Disability. 10(3) pp141-149.
https://doi.org/10.3233/TAD-1999-10302
40. Gitlan LN, Corcoran M, Winter L, Boyce A, Hauck WW. (2001) A randomized controlled
trial of a home environmental intervention: Effect on efficacy and upset in caregivers
and on daily function of persons with dementia, Gerontologist, 41(1) pp4-22.
https://doi.org/10.1093/geront/41.1.4

29
41. Gitlan LN (2003). Conducting Research on Home Environments: Lessons Learned and
New Directions. The Gerontologist, 43(5) pp628-637.
https://doi.org//10.1093/geront/43.5.628
42. Hammel J, Lai J, Heller T. (2002) The impact of assistive technology and environmental
interventions on function and living situation status with people who are ageing with
developmental disabilities, Disabil Rehabil, 24:( 1-3) pp93-105.
https://doi.org/10.1080/09638280110063850
43. Healthy Housing Solutions (2017) Overcoming Obstacles to Policies for Preventing Falls
by the Elderly, Final Report, Prepared for Office of Lead Hazard Control and Healthy
Homes, HUD, Contract #DU203NO-15-D-06, Order #004
https://www.hud.gov/sites/documents/OVERCOMINGOBSTACLESFALLS.PDF and
https://www.hud.gov/sites/dfiles/HH/documents/SeniorFalls_Toolkit.pdf
44. Heywood F. (2001) Money well spent, Bristol: Joseph Rowntree Foundation, The Policy
Press
45. Heywood F, Turner L. (2007) Better outcomes, lower cost: implications for health and
social care budgets of investment in housing adaptations, improvements and
equipment. London: ODI
46. Holly, R. (2021). [Updated] SNF-Diversion Bill ‘Choose Home’ Introduced, Projected to
save up to $247M Annually. Home Health Care News.
https://homehealthcarenews.com/2021/07/snf-diversion-bill-choose-home-introduced-
projected-to-save-up-to-247m-annually/?euid=5874ee70c8&utm_source=hhcn-
newsletter&utm_medium=email&utm_campaign=4485f46263
47. HomeAdvisor (2021). How much does it cost to remodel for disability accommodation?
https://www.homeadvisor.com/cost/environmental-safety/remodel-for-disability-
accommodation/
48. Hornbrook MC, Stevens VJ, Wingfield DJ, Hollis JF, Greenlick MR, Ory MG (1994)
Preventing falls among community-dwelling older persons: results from a randomized
trial, Gerontologist, 34(1) pp16-23. https://doi.org/10.1093/geront/34.1.16
49. Howden LM, Meyer JA (2011) Age and Sex Composition: 2010, US Census Bureau,
https://www.census.gov/prod/cen2010/briefs/c2010br-03.pdf
50. HUD (2013) Aging in Place: Facilitating Choice and Independence, Fall 2013, Office of
Policy Development and Research, US Department of Housing and Urban Development.
https://www.huduser.gov/portal/periodicals/em/fall13/highlight1.html
51. Hwang E, Cummings L, Sixsmith A, Sixsmith J. (2011) Impacts of home modifications on
aging-in-place, J Hous Elder, 25 pp246-257.
https://doi.org/10.1080/02763893.2011.595611
52. IMPAQ International (2019) Housing Upgrades to Benefit Seniors: Efficiency, Impact and
Replication Evaluation. https://civicworks.com/wp-content/uploads/2019/01/HUBS-
Final-Report_March2019.pdf
53. Inzitari M, Risco E, Cesari M, Buurman BM, Kuluski K, Davey V, Bennett L, Varela J, Prvu
Bettger J (2020) Nursing Homes and Long Term Care After COVID-19: A New Era, J Nutri
Health Aging, 24, pp 1042-1046. https://doi.org/10.1007/s12603-020-1447-8
54. Joint Center for Housing Studies at Harvard University. (2016). Projections and
Implications for Housing a Growing Population: Older Households 2015-2035.

30
https://www.jchs.harvard.edu/sites/default/files/harvard_jchs_housing_growing_popul
ation_2016_1_0.pdf
55. Joint Center for Housing Studies at Harvard University (2019a) Improving America’s
Housing.
https://www.jchs.harvard.edu/sites/default/files/reports/files/Harvard_JCHS_Improving
_Americas_Housing_2019.pdf
56. Joint Center for Housing Studies at Harvard University (2019b) Projections and
Implications for Housing a Growing Population: Older Households 2015-2035.
https://www.jchs.harvard.edu/research-areas/reports/projections-and-implications-
housing-growing-population-older-households
57. Joint Center for Housing Studies at Harvard University (2021) Improving America’s
Housing 2021. https://www.jchs.harvard.edu/improving-americas-housing-2021
58. Jones A, de Jonge D, Phillips R (2008) The Impact of home maintenance and
modification services on health, community care and housing outcomes in later life,
Australian Housing and Urban Research Institute, #103 https://apo.org.au/node/914
59. Jutkowitz E, Gitlin LN, Pizzi LT, Lee E, Dennis MP. (2013) Cost effectiveness of a home-
based Intervention that helps functionally vulnerable older adults age in place at home,
J Aging Research, 2012:Article ID 680265. https://doi.org/10.1155/2012/680265
60. Kamei T, Kajii F, Yamamoto Y, Irie Y, Kozakai R, Sugimoto T, Chigira A, Niino N. (2015)
Effectiveness of a home hazard modification program for reducing falls in urban
community-dwelling older adults: a randomized controlled trial, Jpn J Nurs Sci, 12
pp184-197. https://doi.org/10.1111/jjns.12059
61. Keall MD, Pierse N, Howden-Chapman P, Cunningham C, Cunningham M, Guria J, Baker
MG. (2015) Home Modifications to Reduce Injuries from falls in the Home Injury
Prevention Intervention (HIPI) study: a cluster-randomised controlled trial, The Lancet,
385 pp231-238. https://doi.org/10.1016/S0140-6736(14)61006-0
62. Kochera, A. (2002) Falls Among Older Persons and the Role of the Home: An Analysis of
Cost, Incidence, and Potential Savings from Home Modification, AARP Public Policy
Institute, March 2002. https://www.aarp.org/home-garden/home-improvement/info-
2002/aresearch-import-788-IB56.html
63. Lam K, Shi Y, Boscardin J, Covinsky KE (2021) Unmet Need for Equipment to Help with
Bathing and Toileting Among Older US Adults, JAMA Intern Med,
https://doi.org/10.1001/jamainternmed.2021.0204
64. Landers S, Madigan E, Leff B, Rosati RJ, McCann BA, Hornbake R, MacMillan R, Jones K,
Bowles K, Dowding D, Lee T, Moorhead T, Rodriguez S, Breese E (2016) The Future of
Home Health Care: A Strategic Framework for Optimizing Value, Home Health Care
Mgmt & Prac, 28(4) pp262-278. https://doi.org/10.1177/1084822316666368
65. Leff, B. (2021). Aging Media, April 5, 2021. https://vision.agingmedia.com/dr-bruce-
leff/
66. Lieber,R. (2020) An Oral History of the World’s Biggest Coupon, New York Times,
December 19, 2020, https://nyti.ms/3mCTVaV
67. Lin MR, Wolf SL, Hwang HF, Gong SY, Chen CY. (2007) A randomized, controlled trial of
fall prevention programs and quality of life in older fallers, J Am Geriatr Soc, 55(4)
pp499-506 10.1111/j.1532-5415.2007.01146.x

31
68. Ling C, Henderson S, Henderson R, Henderson M, Petro T, Pang L (2008) Cost benefit
considerations of preventing elderly falls through environmental modifications to
homes in Hana, Maui, Hawaii Med J, 67(3) pp65-68
69. Liu SY, Lapane KI. (2009) Residential Modifications and Decline in Physical Function
Among Community-Dwellingn Older Adults, The Gerontologist, 49(3) pp344-354.
https://doi.org/10.1093/geront/gnp033
70. Lord SR, Menz HB, Sherrington C. (2006). Home Environment risk factors for falls in
people and the efficacy of home modifications. Age and Ageing 2006; 35-S2: ii55-ii59.
https://doi.org/10.1093/ageing/afl088
71. MacKillop E, Sheard S (2018) Quantifying life: Understanding the history of Quality-
Adjusted Life-Years (QALYs), Soc Sci & Med, 211 pp 359-366
https://doi.org/10.1016/j.socscimed.2018.07.004
72. Mann WC, Ottenbacher JK, Fraas L, Tomita M, Granger CV (1999) Effectiveness of
assistive technology and environmental interventions in maintaining independence and
reducing home care costs for the frail elderly: A randomized controlled trial, Archives of
Family Medicine, 8 pp210-217. https://doi.org/10.1001/archfami.8.3.210
73. Marseille E, Larson B, Kazi DS, Kahn JG, Rosen S (2014) Thresholds for the cost-
effectiveness of interventions: alternative approaches, Bull World Health Organ, 93
pp118-124 https://doi.org/10.2471/BLT.14.138206
74. Mathews AW, McGinty T (2020) Covid Spurs Families to shun Nursing Homes, a Shift
that Appears Long Lasting, Wall Street Journal, December 21, 2020.
https://www.wsj.com/articles/covid-spurs-families-to-shun-nursing-homes-a-shift-that-
appears-long-lasting-11608565170
75. McMaster University (2018) Adapting your home to age in place. May 23, 2018.
https://www.mcmasteroptimalaging.org/blog/detail/blog/2018/05/23/adapting-your-
home-to-age-in-place
76. Medina L, Sabo S, Vespa J (2020) Living Longer: Historical and Projected Life Expectancy
in the United States, 1960 to 2060: Population Estimates and Projections, Current
Population Reports, P25-1145, February 2020,
https://www.census.gov/content/dam/Census/library/publications/2020/demo/p25-
1145.pdf
77. Meucci MR, Gozalo P, Dosa D, Allen SA. (2016) Variation in the Presence of Simple Home
Modifications of Older Americans: Findings from the National Health and Aging Trends
Study, J Am Geriatr Soc, 64(10) pp2081-2087. https://doi.org/10.1111/jgs.14252
78. Mitoku K, Shimanouchi S (2014) Home modification and prevention of frailty
progression in older adults: a Japanese prospective cohort study, J Gerontol Nurs, 40(8),
pp40-47. https://doi.org/10.3928/00989134-20140311-02
79. Molinsky JH, Herbert C (2020) Can the Nation’s Housing Support a Population Seeking to
Age in Place?, Generations Journal, https://generations.asaging.org/older-adults-aging-
place-affordable-safe
80. Munnell AH, Walters AN, Belbase A, Hou W (2020). Are Homeownership Patterns Stable
Enough to Tap Home Equity? Center for Retirement Research at Boston College WP
2020-7. https://crr.bc.edu/wp-content/uploads/2020/02/wp_2020-7_.pdf

32
81. Naik AD, Gill T (2005) Underutilization of environmental adaptations for bathing in
community-living older persons, J Am Geriatr Soc, September, 2005, 53(9) pp1497-1503.
https://doi.org/10.1111/j.1532-5415.2005.53458.x
82. Neumann PJ, Cohen JT, Weinstein MC (2014) Updating Cost-Effectiveness – The Curious
Resilience of the $50,000-per-QALY Threshold, N Engl J Med, 371(9) pp 796-797
https://doi.org/10.1056/NEJMp1405158
83. Newman SJ, Struyk R, Wright P, Rice M. (1990) Overwhelming odds: caregiving and the
risk of institutionalization, J Gerontol, September, 1990, 45(5) ppS173-S183.
https://doi.org/10.1093/geronj/45.5.s173
84. Nikolaus T, Bach M (2003) Preventing Falls in Community-Dwelling Frail Older People
Using a Home Intervention Team (HIT): Results from the Randomized Falls-HIT Trial, J
Am Geriatr Soc, 51(3) pp 300-305. https://doi.org/10.1046/j.1532-5415.2003.51102.x
85. Noonan RK, Sleet DA, Stevens JA (2011) Closing the gap: a research agenda to
accelerate the adoption and effective use of proven older adult fall prevention
strategies, J Safety Res, 42(6) pp427-30 https://doi.org/10.1016/j.jsr.2010.12.002
86. Olij BF, Ophuis RH, Polinder S, van Beeck EF, Burdorf A, Panneman MJM, Sterke CS
(2016) Economic Evaluations of Falls Prevention Programs for Older Adults: A Systematic
Review, J Am Geriatr Soc, 66(11) pp 2197-2204. https://doi.org/10.1111/jgs.15578
87. Palvanen M, Kannus P, Piirtola M, Niemi S, Parkkari J, Jarvinen M (2014). Effectiveness of
the Chaos Falls Clinic in preventing falls and injuries of home-dwelling older adults: A
randomized controlled trial. Injury, Int. J. Care Injured. 45(1) pp 265-271.
https://doi.org/10.1016/j.injury.2013.03.010
88. Pearson CF, Quinn CC, Loganathan S, Datta AR, Mace BB, Brabowski DC. (2019) The
Forgotton Middle: Many Middle-Income Seniors Will Have Insufficient Resources for
Housing and Health Care, Health Affairs, 38(5) pp851-859.
https://doi.org/10.1377/hlthaff.2018.05233
89. Peel N, Steinberg M, Williams G. (2000) Home safety assessment in the prevention of
falls among older people. Aus and NZ J of Pub Health, 2000 24(5), pp 536-539.
https://onlinelibrary.wiley.com/doi/epdf/10.1111/j.1467-842X.2000.tb00506.x
90. Pega F, Kvizhinadze G, Blakely T, Atkinson J, Wilson N (2016) Home Safety assessment
and modification to reduce injurious falls in community-dwelling older adults: cost-utlity
and equity analysis, Inj Prev 22(6) pp 420-426. https://doi.org/10.1136/injuryprev-2016-
041999
91. Petersson I, Lilja M, Hammel J, Kottorp A. (2008) Impact of home modification services
on ability in everyday life for people ageing with disabilities, J Rehabil Med, 40 pp253-
260. https://doi.org/10.2340/16501977-0160
92. Piatkowski M, Abushousheh A, Taylor E (2019) Healthcare at Home: A White Paper
Supporting The Center for Heath Design Interactive Diagrams, The Center for Heath
Design.
https://www.healthdesign.org/system/files/res_files/White%20Paper_Healthcare%20at
%20Home_2019_0.pdf
93. Pifer R, (2021) Support for telehealth Medicare reimbursement gains steam in Congress,
March 3, 2021, https://www.healthcaredive.com/news/house-backing-for-telehealth-
medicare-reimbursement-gains-steam/596013/

33
94. Pighills AC, Torgerson DJ, Sheldon TA, Drummond AE, Bland JM (2011) Environmental
Assessment and Modification to Prevent Falls in Older People. J Am Geriatr Soc, January
2011, 59(1), pp 26-33. https://doi.org/10.1111/j.1532-5415.2010.03221.x
95. Plautz B, Beck DE, Selmar C, Radetsky M (1996) Modifying the environment: a
community-based injury-reduction program for elderly residents, Am J Prev Med, 12(4
Supp) pp33-38.
96. Powell J, Mackintosh S, Bird E, Ige J, Garrett H, Roys M (2017) The role for home
adaptations in improving later life, Centre for Ageing Better University of the West of
England, November 2017. https://www.ageing-better.org.uk/publications/role-home-
adaptations-improving-later-life
97. Public Health Administration Australia (2019) Fall Injury Prevention in Older Policy
Position Statement. https://www.phaa.net.au/documents/item/3811
98. Ruiz S, Snyder LP, Rotondo C, Cross-Barnet C. (2016) Innovative Home Visit Models
Associated with Reductions in Costs, Hospitalizations, and Emergency Department Use,
Health Affairs, 36(3) pp425-432. https://doi.org/10.1377/hlthaff.2016.1305
99. Safran-Norton CE. (2010) Physical Home Environment as a Determinant of Aging in Place
for Different Types of Elderly Households, J Hous Elder, 24(2) pp208-231
https://doi.org/10.1080/02763891003757494
100. Salkeld G, Cumming RG, Thomas M, Szonyi G, Westbury C, O’Neill E. (2000) The
cost effectiveness of a home hazard reduction program to reduce falls among older
persons, Aust J Z J Public Health, 24(3) pp 265-271. https://doi.org/10.1111/j.1467-
842x.2000.tb01566.x
101. Salmen JPS, (1991) The Do-Able Renewable Home: Making Your Home Fit Your
Needs, Revised and Reprinted by the Pennsylvania Housing Finance Agency with
authority from AARP. http://www.family-friendly-
fun.com/documents/doable_renewable_home.pdf
102. Sheffield C, Smith CA, Becker M. (2013) Evaluation of an agency-based
occupational therapy intervention to facilitate aging in place. Gerontologist, 53(6)
pp907-918. https://doi.org/10.1093/geront/gns145
103. Smith RD, Wdiatmoko D (1998) The cost-effectiveness of home assessment and
modification to reduce falls in the elderly, Aust N Z J Public Health, 22(4) pp436-40.
https://onlinelibrary.wiley.com/doi/epdf/10.1111/j.1467-842X.1998.tb01410.x
104. Spader J (2019). Tenure Projections of Homeowner and Renter Households for
2018-2038. Joint Center for Housing Studies. March 2019.
https://www.jchs.harvard.edu/sites/default/files/media/imp/Harvard_JCHS_Spader_Te
nure_Projections_2018-2038.pdf
105. Stark S, Landsbaum A, Palmer JL, Somerville, EK, Morris JC. (2009) Client-centred
home modifications improve daily activity performance of older adults. Can J Occup
Ther, 76 pp235-245. https://doi.org/10.1177/000841740907600s09
106. Stark S, Keglovits M, Arbesman M, Lieberman D (2017) Effect of Home
Modification Interventions on the Participation of Community-Dwelling Adults with
Health Conditions: A Systematic Review, Am J Occup Th, 71(2), pp 7102290010p1-
7102290010p11 https://doi.org/10.5014/ajot.2017.018887
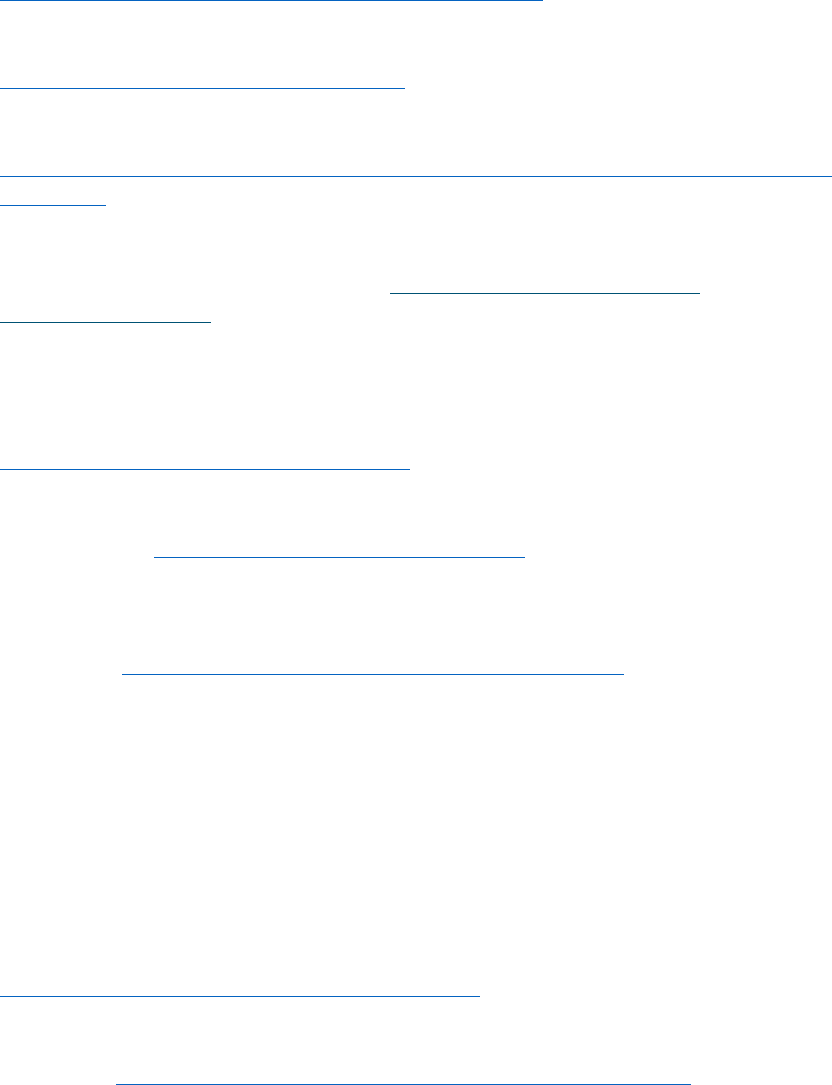
34
107. Stark S, Keglovitz M, Somerville E, Hu YL, Barker A, Sykora D, Yan Y (2021) Home
Hazard Removal to Reduce Falls Among Community-Dwelling Older Adults A
Randomized Clinical Trial, JAMA Network Open, 4(8):e2122044.
https://doi.org/10.1001/jamanetworkopen.2021.22044
108. Stevens JA, (2005) Falls among older adults – risk factors and prevention
strategies. J of Safety Research, 36 (4) pp 409-411
https://doi.org/10.1016/j.jsr.2005.08.001
109. Stevens JA, Burns E (2015) A CDC Compendium of Effective Fall Interventions:
What Works for Community-Dwelling Older Adults.
https://www.cdc.gov/homeandrecreationalsafety/pdf/falls/CDC_Falls_Compendium-
2015-a.pdf
110. Stevens M, D’Arcy C, Holman J, Bennett N, de Klerk N (2001) Preventing Falls in
Older People: Outcome Evaluation Randomized Controlled Trial. J Am Geriatr Soc.
49(11). November 2001. pp 1448-1455. https://doi.org/10.1046/j.1532-
5415.2001.4911236.x
111. Szanton SL, Wolff JW, Leff B, Thorpe RJ, Tanner EK, Boyd C, Xue Q, Guralnik J,
Bishai D, Gitlin LN (2014) CAPABLE trial: a randomized controlled trial of nurse,
occupational therapist and handyman to reduce disability among older adults: rationale
and design, Contemp Clin Trials, 38(1) pp 102-112.
https://doi.org/10.1016/j.cct.2014.03.005
112. Szanton SL, Gitlin LN (2016) Meeting the Health Care Financing Imperative
Through Focusing on Function: The CAPABLE Studies. Public Policy and Aging Report,
26(3), 106-110. https://doi.org/10.1093/ppar/prw014
113. Szanton SL, Xue QL, Leff B, Guralnik J, Wolff JL, Tanner EK, Boyd C, Thorpe RJ,
Bishai D, Gitlin LN (2019) Effect of a Biobehavioral Environmental Approach on Diability
Among Low-Income Older Adults: A Randomized Clinical Trial, JAMA Intern Med, 179(2)
pp 204-211 https://doi.org/10.1001/jamainternmed.2018.6026
114. Tenenbaum L, (2010) The MetLife Report on Aging in Place 2.0: Rethinking
Solutions to the Home Care Challenge, MetLife Mature Market Institute.
115. Thaler RH, Sunstein CR. (2008) Nudge: Improving Decisions About Health, Wealth
and Happiness, Penguin Books: London
116. Tinetti ME, Baker BI, McAvay G, Claus EB, Garrett P, Gottschalk M, Koch ML,
Trainor K, Horowitz RI. (1994) A Multifactorial Intervention to Reduce the Risk of Falling
Among Elderly People Living in the Community. NE J of Med, September 29, 1994,
331(13), pp 821-827 10.1056/NEJM199409293311301
117. Tinetti ME, Williams CS (1997) Falls, injuries due to falls, and the risk of
admission to a nursing home, N Engl J Med, 337(18) pp1279-84
https://doi.org/10.1056/NEJM199710303371806
118. Todd M, Pressley K, Pharis M (2020) The burden of serious falls among older
adults in Philadelphia PA, presented at the GSA Annual Meeting November 4-7, 2020,
mimeo and https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7742999/
119. Turner S, Arthur G, Lyons RA, Weightman AL, Mann MK, Jones SJ, John A, Lannon
S (2011) Modification of the home environment for the reduction of injuries, Cochrane

35
Database of Systematic Reviews, Issue 2. Art. No.:CD003600
https://doi.org/10.1002/14651858.CD003600.pub3
120. US Bureau of Economic Analysis, (2017) Picking the Right Health Care Price
Index. https://www.bea.gov/news/blog/2017-05-19/picking-right-health-care-price-
index
121. US Census Bureau (2021) 2019 American Housing Survey.
https://www.census.gov/programs-
surveys/ahs/data/interactive/ahstablecreator.html?s_areas=00000&s_year=2019&s_ta
blename=TABLE8B&s_bygroup1=1&s_bygroup2=10&s_filtergroup1=1&s_filtergroup2=1
122. US Preventive Service Task Force (2018) Interventions to Prevent Falls in
Community-Dwelling Older Adults Recommendation Statement.
https://doi.org/10.1001/jama.2018.3097
123. US Preventive Services Task Force,
https://www.uspreventiveservicestaskforce.org/uspstf/about-uspstf
124. Vespa J, Engelberg J, He W (2020) Old Housing, New Needs: Are U.S. Homes
Ready for an Aging Population? US Census Bureau Current Population Reports, P23-217,
May 2020.
https://www.census.gov/content/dam/Census/library/publications/2020/demo/p23-
217.pdf
125. Vespa J, Medina L, Armstrong DM, (2018) Demographic Turning Points for the
United States: Population Projections for 2020 to 2060, Current Population Reports P25-
1144, US Census Bureau,
https://www.census.gov/library/publications/2020/demo/p25-1144.html
126. Warren, C. & Lindberg, C. & Hansen, M. & Pittman, B. (2016). An Assessment of
Home Renovation and Rehabilitation Needs of Older Adult Homeowners in Minnesota:
Estimates of Need and Costs for Minnesota Housing and Minnesota Department of
Human Services, Wilder Research.
https://www.wilder.org/sites/default/files/imports/MNHousing_CostsOfHomeRehabAn
dImprovement_%2012-16.pdf
127. Will A (2015) Aging in Place: Implications for Remodeling, Joint Center for
Housing Studies, Harvard University, W15-4.
https://www.jchs.harvard.edu/sites/default/files/w15-4_will_1.pdf
128. Wilson DJ, Mitchell JM, Kemp BJ, Adkins RH, Mann W. (2009) Effects of assistive
technology on functional decline in people aging with a disability. Assist Technol, 21(4)
pp208-217. https://doi.org/10.1080/10400430903246068
129. World Health Organization (2008) WHO Global Report on Falls Prevention in
Older Age. https://www.who.int/publications/i/item/9789241563536
130. World Health Organization (2018) WHO Housing and Health Guidelines.
https://www.who.int/publications/i/item/9789241550376
