
J.
Phypiol.
(1975),
250,
pp.
431-441
431
With
3
text-ftgurew
Printed
in
Great
Britain
MUSCULAR
REFLEX
STIMULI
TO
THE
CARDIOVASCULAR
SYSTEM
DURING
ISOMETRIC
CONTRACTIONS
OF
MUSCLE
GROUPS
OF
DIFFERENT
MASS
BY
D.
I.
McCLOSKEY
AND
K.
A.
STREATFEILD
From
the
School
of
Physiology
and
Pharmacology,
University
of
New
South
Wales,
Post
Office
Box
1,
Kensington
2033,
Sydney,
Australia
(Received
13
February
1975)
SUMMARY
1.
The
cardiovascular
responses
to
voluntary
isometric
contractions
performed
by
human
subjects
are
determined
by
the
proportion
of
maxi-
mal
tension
achieved
by
the
muscles
contracting,
and
not
by
the
mass
of
the
contracting
muscles,
nor
by
the
absolute
tension
achieved
(Lind
&
McNicol,
1967;
confirmed
here).
When
two
or
more
muscle
groups
contract
simultaneously
at
different
relative
tensions,
the
increments
in
heart
rate
and
blood
pressure
are
the
same
as
when
the
muscle
group
at
the
higher
relative
tension
contracts
alone
at
that
tension
(Lind
&
McNicol,
1967).
It
is
known
that
there
are
both
central
and
reflex
stimuli
to
the
cardio-
vascular
system
in
exercise,
and
the
present
study
examines
whether
the
muscular
reflex
stimuli
are
related
to
the
proportion
of
maximal
tension
achieved
or
to
the
mass
of
contracting
muscle.
2.
Isometric
hind-limb
contractions
were
induced
in
anaesthetized
dogs
and
cats
by
stimulation
of
spinal
ventral
roots.
Pressor
responses
to
contraction
of
both
hind
limbs
were
greater
than
responses
to
contractions
of
either
hind
limb
alone.
No
differences
were
observed
between
heart
rate
responses
to
single
or
combined
hind-limb
contractions.
3.
When
human
subjects
perform
isometric
contractions,
a
pressor
re-
sponse
can
be
maintained
beyond
the
conclusion
of
the
exercise
by
occluding
muscle
blood
flow.
This
response
is
generally
attributed
to
a
reflex
set
up
in
the
muscle
by
the
action
of
chemical
factors
on
afferent
nerves.
When
comparable
pressor
responses
were
evoked
by
comparable
proportional
efforts
with
either
the
whole
hand
or
the
little
finger,
it
was
found
here
that
the
pressor
responses
remaining
during
the
period
of
post-exercise
occlusion
were
greater
when
the
greater
mass
of
muscle
had
been
exercised.
4.
It
is
concluded
that
the
muscular
reflex
drive
in
isometric
exercise
is
related
to
the
bulk
of
contracting
muscle.

D.
I.
McCLOSKEY
AND
K.
A.
STREATFEILD
INTRODUCTION
When
human
subjects
perform
sustained
hand-grip
contractions
at
tensions
above
15
%
of
the
maximum
attainable,
the
heart
rate,
cardiac
output,
and
systolic
and
diastolic
arterial
pressures
all
increase,
and
the
magnitude
of
these
increases
is
determined
by
the
intensity
of
the
con-
traction
and
its
duration
(Lind,
Taylor,
Humphreys,
Kennelly
&
Donald,
1964).
It
has
been
suggested
that
the
physiological
advantage
of
these
responses
is
the
increased
flow
which
is
possible
in
the
contracting
muscle
group
when
the
blood
pressure
rises
(Humphreys
&
Lind,
1963).
There
are
certain
peculiar
features
of
the
cardiovascular
responses
to
such
isometric
contractions.
For
example,
when
two
or
more
muscle
groups
contract
at
the
same
proportion
of
their
maximal
tension,
the
increments
in
blood
pressure
and
heart
rate
are
the
same
whether
they
contract
separately
or
together
(Lind
&
McNicol,
1967).
Or,
when
two
or
more
muscle
groups
contract
simultaneously
at
different
relative
tensions,
the
increments
in
heart
rate
and
blood
pressure
are
the
same
as
when
the
muscle
group
at
the
higher
relative
tension
contracts
alone
at
that
tension
(Lind
&
McNicol,
1967).
These
findings
hold
true
even
when
the
muscle
groups
involved
are
of
quite
different
total
mass.
Isometric
exercise
has
been
used
in
experiments
on
the
nature
of
the
stimuli
to
the
cardiovascular
system
in
exercise.
These
stimuli
include
'irradiation'
of
the
cardiovascular
control
centres
by
elements
of
the
command
signals
descending
from
higher
centres
to
the
contracting
muscles
(Goodwin,
McCloskey
&
Mitchell,
1972),
and
reflex
stimuli
origi-
nating
in
nerve
endings
in
the
contracting
muscles
(Coote,
Hilton
&
Perez-Gonzalez,
1971;
McCloskey
&
Mitchell,
1972).
It
is
not
known
whether
both
central
and
reflex
stimuli
are
related
to
the
proportion
of
maximal
tension
achieved
rather
than
to
the
mass
of
muscle
involved
in
the
contraction.
Nor
is
it
known
whether
these
two
components
of
the
cardiovascular
drive
contribute
similarly
in
similar
relative
contractions
of
different
muscle
groups.
In
the
present
study
the
reflex
contributions
to
the
cardiovascular
drives
during
isometric
contractions
of
muscle
groups
of
different
masses
have
been
investigated
in
animals
and
in
man.
In
the
animal
experiments
isometric
contractions
of
hind-limb
muscles
were
induced
by
spinal
ventral
root
stimulation,
as
this
allows
the
reflex
part
of
the
cardiovascular
drive
to
be
seen
alone.
In
the
experiments
on
human
subjects,
reflex
circulatory
effects
were
investigated
by
using
occlusion
of
the
blood
supply
to
the
contracting
muscle.
This
causes
the
maintenance
of
a
pressor
response
beyond
the
conclusion
of
the
exercise
for
as
long
as
the
occlusion
persists
(Alam
&
Smirk,
1937).
This
is
generally
attributed
to
a
reflex
set
up
in
the
432

EXERCISE
REFLEXES43
ischaemic
muscle
by
the
action
of
chemical
factors
on
sensory
nerve
endings.
Such
a
reflex
is
probably
part,
and
perhaps
the
whole,
of
the
muscular
reflex
element
of
the
cardiovascular
drive
in
exercise,
and
can
be
observed
when
it
is
the
sole
drive
to
the
cardiovascular
system.
Our
results
indicate
that
the
muscular
reflex
component
of
the
cardiovascular
stimulus
in
isometric
exercise
is
related
to
the
mass
of
the
muscle
group
performing
the
contraction.
METHOD
Animal
experiments
Experiments
were
performed
on
nine
cats
(1.8-3.8
kg)
anaesthetized
with
pento-
barbitone
sodium
(Nembutal:
Abbott,
40
mg/kg,
i.r.),
and
on
six
dogs
(6-14
kg)
anaesthetized
with
chloralose
(ac-chloralose:
British
Drug
Houses,
80
mg/kg
v.v.),
after
thiopentone
induction.
A
tracheal
cannula
was
inserted
low
in
the
neck.
Blood
pressure
was
recorded
from
the
axillary
artery
through
a
saline-filled
nylon
catheter
connected
to
a
Statham
P23AC
transducer,
and
was
recorded
on
a
Grass
polygraph
pen
recorder.
On
another
channel
of
this
recorder
either
the
electrocardiogram
or
heart
rate
was
recorded
using
a
Grass
5P4D
pre-amplifier.
A
laminectomy
was
performed
to
expose
the
sacral
and
lower
lumbar
segments
of
the
spinal
cord.
Animals
were
fixed
in
a
prone
position
on
a
table
by
pins
driven
into
the
iliac
crests
and
through
the
knee
joints,
and
the
ankle
joints
were
firmly
clamped
to
prevent
movement.
A
pool
was
made
over
the
laminectomy
with
para-
ffin
warmed
to
370
C
and
bubbled
with
95
%
02
+
5
%
C02.
The
spinal
cord
was
exposed
by
a
lengthwise
incision
through
the
dura.
The
ventral
roots
of
L
6,
L
7
and
occasionally
S
1
were
cut
close
to
their
exit
from
the
spinal
cord
on
each
side
and
were
placed
over
pairs
of
Ag-AgCl
electrodes.
Stimulation
of
the
ventral
roots
at
20-50
Hz
with
square
wave
pulses
of
0-2-0-5
msec
duration,
delivered
by
an
isolated
stimulator,
were
used
to
elicit
sustained
isometric
contractions
of
the
hind-
limb
muscles.
The
voltage
used
for
maximal
contractions
was
twice
motor
threshold.
Periods
of
contraction
of
10-40
see
were
used.
The
exposed
spinal
cord
and
nerve
roots
were
washed
every
30-40
min
with
warmed
Ringer
solution
bubbled
with
95%
02
+
5%
C02
(cf.
Brown,
Lawrence
&
Matthews,
1969).
Rectal
temperatures
were
maintained
at
36-38°
C
throughout.
Human
experiments
Ten
normal
volunteer
subjects
(eight
male
and
two
female),
aged
between
19
and
26
yr,
acted
as
experimental
subjects.
The
experiments
were
performed
with
the
understanding
and
consent
of
the
subjects.
Subjects
were
required
to
perform
isometric
contractions
using
muscle
groups
of
the
preferred
hand
or
forearm.
Usually,
handgrip
contractions
and
'trigger-pulling'
contractions
of
the
little
finger
of
the
same
hand
were
compared.
Three
subjects
per-
formed
combined
contractions
of
the
index
and
middle
finger
of
the
same
hand,
attempting
to
close
the
extended
digits
in
a
scissors-like
action
on
the
strain
gauge:
this
form
of
contraction,
when
undertaken,
was
used
instead
of
the
contraction
of
the
little
finger
for
comparison
with
the
hand-grip.
Contractions
were
performed
at
about
40
%
of
the
maximal
voluntary
tension
for
1-1
min.
Handgrip
contractions
alternated
with
contractions
of
the
smaller
muscle
group,
and
there
were
rest
periods
of
at
least
10
min
between
contractions.
During
contractions
the
subject
could
see
only
the
tension
gauge
against
which
he
was
pulling,
and
the
face
of
an
oscilloscope
on
which
were
displayed
the
achieved
tension
and
a
target
beam
for
alignment.
433

D.
I.
McCLOSKEY
AND
K.
A.
STREATFEILD
All
other
equipment,
and
the
experimenters,
were
out
of
sight,
and
the
room
was
kept
silent.
Five
seconds
before
the
conclusion
of
each
contraction
a
sphygmomano-
meter
cuff
was
inflated
above
the
elbow
on
the
experimental
side
to
a
pressure
of
250
mmHg,
and
was
kept
inflated
after
the
conclusion
of
the
effort
for
a
further
1-1
min.
The
first
contiaction
in
a
series
was
always
neglected
for
purposes
of
analysis,
and
served
only
to
familiarize
the
subject
with
the
experimental
pro-
cedure.
Blood
pressure
was
measured
continuously
through
a
short
Teflon
catheter
in-
serted
through
the
skin
into
the
radial
artery
of
the
resting
arm.
This
catheter
was
connected
to
a
Statham
P23Dc
transducer,
and
blood
pressure
was
recorded
on
a
Grass
polygraph
pen
recorder.
Heart
rate
was
obtained
through
a
Grass
5P4D
pre-
amplifier
from
the
radial
pulse,
and
was
also
recorded.
The
tension
achieved
during
the
isometric
effort
was
recorded
on
a
third
channel
of
the
polygraph.
RESULTS
Animal
experiments
In
all
the
animal
experiments
the
pressor
and
heart-rate
responses
to
maximal
induced
contractions
of
one
hind
limb
alone
were
compared
with
the
responses
to
maximal
contractions
of
both
hind
limbs
together.
In
all
but
two
experiments
the
pressor
response
to
combined
contractions
exceeded
the
response
to
contraction
of
either
limb
contracting
alone.
In
these
thirteen
experiments
the
maximal
increase
in
blood
pressure
on
contraction
of
a
single
hind
limb
ranged
from
10
to
35
mmHg
for
individual
animals,
and
the
maximal
pressor
response
for
combined
hind-limb
con-
tractions
ranged
from
20
to
50
mmHg.
When
the
maximal
increase
in
pressure
for
combined
contractions
was
expressed
as
a
percentage
of
the
maximal
increase
in
response
to
contraction
of
a
single
hind
limb
in
the
same
animal,
the
range
for
individual
experiments
was
150-230
%.
In
the
remaining
two
experiments,
both
done
on
cats,
the
maximal
pressor
responses
to
single
and
combined
hind-limb
contractions
were
of
similar
magnitude:
in
both
experiments
these
were
small
(10
and
15
mmHg).
In
all
experiments,
the
reflex
nature
of
the
responses
observed
was
confirmed
when
the
responses
were
abolished
by
cutting
the
spinal
dorsal
roots
from
L
5
downwards.
After
cutting
the
dorsal
roots
there
were
often
small
transient
changes
in
blood
pressure
at
the
start
of
a
contraction,
possibly
due
to
mechanical
alterations
in
peripheral
resistance,
and
slight
reduc-
tions
in
pressure
at
the
conclusion
of
contractions,
possibly
due
to
reactive
hyperaemia
in
the
exercised
muscle.
Bilateral
ventral
root
stimulation
was
performed
in
two
dogs
and
one
cat
which
had
been
paralysed
with
galla-
mine,
and
this
induced
no
changes
in
blood
pressure
or
heart
rate.
Typical
pressor
responses
to
single
and
combined
hind-limb
contractions
are
shown
in
Fig.
1.
Heart
rate
increased
in
response
to
hind-limb
contractions
in
all
experi-
ments.
The
increases
were
variable
in
magnitude,
and
never
exceeded
20
%
434
EXERCISE
REFLEXES
of
the
resting
heart
rate.
We
were
unable
to
demonstrate
any
differences
between
heart
rate
responses
to
single
or
combined
hind-limb
contractions
in
any
animals.
In
five
experiments
submaximal
limb
contractions
were
investigated.
In
all
five
experiments
(three
cats
and
two
dogs)
there
was
a
smaller
pressor
response
to
a
maximal
contraction
of
one
hind
limb
than
to
a
similar
contraction
of
that
hind
limb
combined
with
a
submaximal
125
75
[
125
r
___
75
S
B.P.
(mmHg)
100
so
-
-
30
sec
m
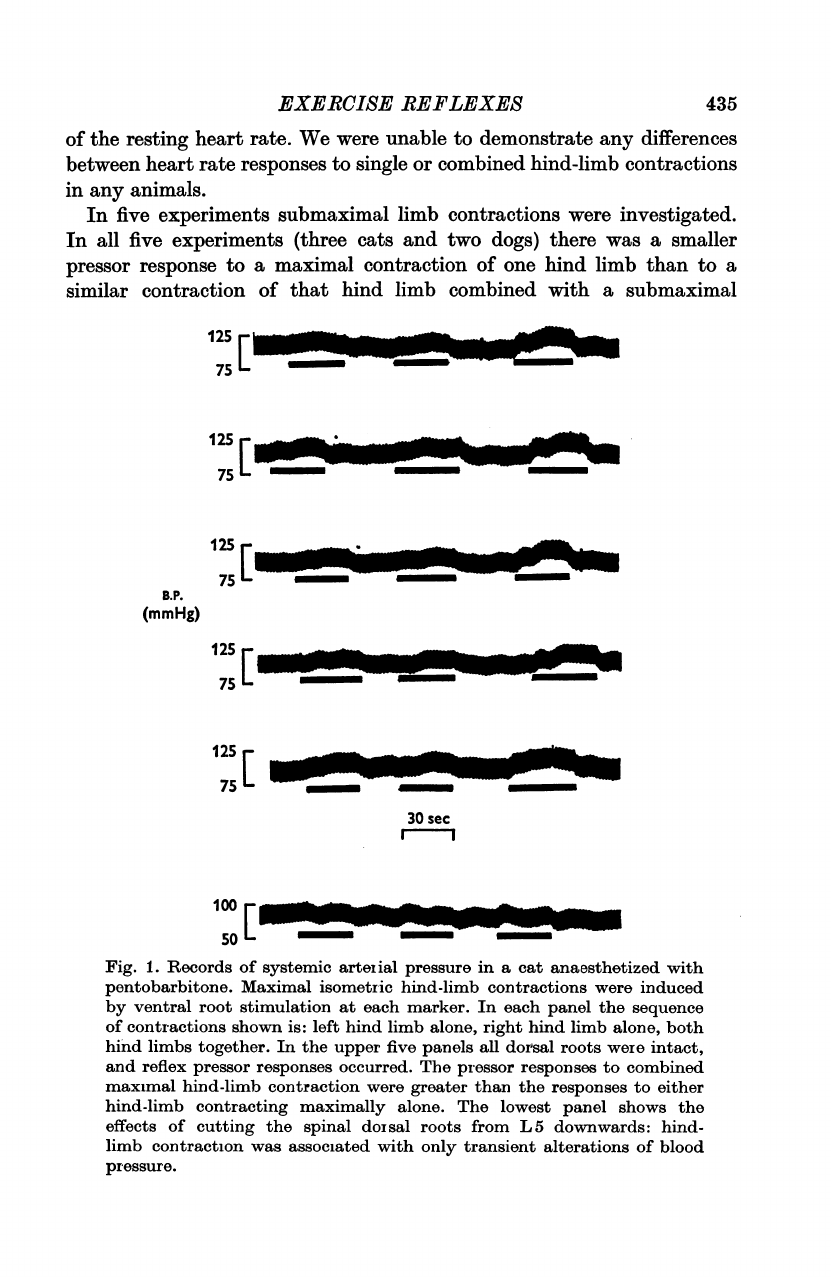
Fig.
1.
Records
of
systemic
arterial
pressure
in
a
cat
anaesthetized
with
pentobarbitone.
Maximal
isometric
hind-limb
contractions
were
induced
by
ventral
root
stimulation
at
each
marker.
In
each
panel
the
sequence
of
contractions
shown
is:
left
hind
limb
alone,
right
hind
limb
alone,
both
hind
limbs
together.
In
the
upper
five
panels
all
dorsal
roots
were
intact,
and
reflex
pressor
responses
occurred.
The
pressor
responses
to
combined
maximal
hind-limb
contraction
were
greater
than
the
responses
to
either
hind-limb
contracting
maximally
alone.
The
lowest
panel
shows
the
effects
of
cutting
the
spinal
dorsal
roots
from
L5
downwards:
hind-
limb
contraction
was
associated
with
only
transient
alterations
of
blood
pressure.
125
W_
75
12S
W_..B
75
435
125S
75L

436
D.
I.
McCLOSKEY
AND
K.
A.
STREATFEILD
contraction
of
the
other
hind
limb.
Fig.
2
shows
typical
responses.
Again
we
were
unable
to
demonstrate
any
relation
between
mass
of
contracting
muscle
and
increase
in
heart
rate
in
any
experiment.
100
I~~~
200
r_"
ba
100
E
30
sec
E
150
50.
Fig.
2.
Records
of
systemic
arterial
pressure
in
a
dog
anaesthetized
with
chloralose.
Hind-limb
contractions
were
induced
by
ventral
root
stimula-
tion
at
each
marker.
The
upper
two
panels
show
reflex
pressor
responses
when
the
dorsal
roots
were
intact.
In
the
top
panel
the
sequence
of
con-
tractions
was:
left
hind
limb
alone,
right
hind
limb
alone,
both
hind
limbs
together;
in
the
second
panel
the
sequence
was
rigbt
hind
limb,
left,
then
both
together.
In
each
sequence
the
left
hind
limb
contracted
maximally
and
the
right
submaximally.
The
pressor
responses
to
combined
maximal
and
submaximal
hind-limb
contraction
were
greater
than
the
responses
to
either
hind-limb
contracting
alone.
The
lowest
panel
shows
the
sequence
of
contractions
of
the
top
panel
repeated
after
cutting
the
spinal
dorsal
roots
from
L
5
downwards.
Human
experiments
Handgrips
and
contractions
of
a
smaller
muscle
group
of
the
same
arm
were
performed
alternately
by
all
subjects,
with
rest
periods
between.
Usually
there
were
three
or
four
contractions
of
each
type.
We
aimed
to
produce
increases
in
systolic
pressure
of
the
same
magnitude
during
each

EXERCISE
REFLEXES
437
form
of
contraction:
this
was
achieved
by
altering
the
magnitude
of
the
effort
required
of
the
smaller
muscle
group.
Handgrip
contractions
of
40
0
of
the
maximal
voluntary
contraction
(MVC)
were
always
used,
and
efforts
producing
similar
pressor
responses
were
within
the
range
35-45
%
MVC
for
the
smaller
muscle
group.
TABLE
1.
Comparison
of
mean
systolic
arterial
pressure
and
heart
rate
response
to
sustained
handgrip
contractions
and
to
contractions
of
smaller
muscle
groups
During
isometric
effort
_
Control
systolic
Control
heart
rate
)ressure
(beats/
Muscle
mmHg)
min)
group
105
65
Hand
Finger
115
76
Hand
Finger
115*
55
Hand
Finger
120
60
Hand
Finger
122
80
Hand
Finger
122
62
Hand
Finger
128*
66
Hand
Finger
134*
85
Hand
Finger
138
72
Hand
Finger
140
68
Hand
Finger
Systolic
pressure
(mmHg)
155
150
140
148
160
160
172
176
156
152
190
182
165
172
184
192
166
170
170
174
Heart
rate
(beats/
mmn)
82
80
95
104
80
74
92
88
124
120
76
82
90
88
104
100
102
110
96
98
During
post-exercise
occlusion
Systolic
Heart
rate
pressure
(beats/
(mmHg)
min)
140
72
112
78
132
70
120
72
134
50
118
56
146
64
130
56
146
86
134
82
178
54
148
56
144
70
138
72
160
90
148
84
152
60
144
62
158
58
148
64
*
All
subjects
used
flexion
of
the
little
finger
as
the
effort
with
a
small
muscle
group,
except
those
marked
*
where
a
scissors-like
contraction
of
the
index
and
middle
fingers
was
employed.
Occlusion
of
the
circulation
through
the
exercising
forearm
was
com-
menced
5
see
before
the
end
of
the
exercise.
When
the
contraction
stopped,
there
was
typically
an
abrupt
fall
in
blood
pressure
and
heart
rate,
which
had
risen
during
the
exercise.
Often
the
blood
pressure
began
to
rise
again
slowly
after
this
initial
fall,
sometimes
stabilizing
some
15-45
see
after
the
(I

D.
I.
McCLOSKEY
AND
K.
A.
STREATFEILD
end
of
the
contraction.
Consistent
changes
were
not
observed
in
heart
rate
during
the
post-exercise
occlusion
period.
We
compared
the
increases
from
control
levels
of
blood
pressure
and
heart
rate
in
the
last
15
sec
of
the
voluntary
effort,
and
between
45
and
60
sec
of
the
post-exercise
occlusion
period.
Table
1
summarizes
the
results.
Systolic
arterial
pressure
in
each
experimental
condition
was
taken
as
the
mean
of
systolic
pressure
throughout
one
or
two
complete
respiratory
175
r
B.P.
I
-
(mmHg)
125
75L
~~L~~~rn
'
5~e
s
H.R.
90
[
(beats/min)
60L
Finger
Hand
I
min
Fig.
3.
Records
of
blood
pressure
and
heart
rate
from
a
normal
human
subject
performing
isometric
contractions.
On
the
left
are
shown
the
responses
to
efforts
made
by
flexing
the
little
finger
at
40
%
of
its
maximal
tension,
and
on
the
right,
the
responses
to
a
handgrip
contraction
at
40
%
of
maximum.
In
each
case
the
duration
of
the
voluntary
effort
is
marked
e.
The
pressor
responses
to
both
efforts
were
comparable
in
size.
Just
before
the
conclusion
of
each
voluntary
effort,
an
occlusion
of
the
blood
supply
through
the
exercising
muscle
was
applied:
the
duration
of
the
period
of
vascular
occlusion
is
marked
c.
During
the
period
of
post-exercise
occlusion
part
of
the
pressor
response
was
maintained.
This
maintained
part
of
the
pressor
response
was
greater
for
the
larger
muscle
group,
as
can
be
seen
by
reference
to
the
line
drawn
across
the
blood
pressure
record.
cycles,
so
as
to
minimize
the
influence
of
respiratory
fluctuations
in
blood
pressure.
In
each
subject
the
mean
of
these
systolic
arterial
pressures,
and
the
mean
heart
rate,
for
the
three
or
four
efforts
in
each
category
were
determined,
and
are
set
out
in
Table
1.
Typical
responses
from
one
subject
are
shown
in
Fig.
3.
In
all
subjects,
the
blood
pressure
was
higher
during
circulatory
occlusion
after
handgrip
contractions
than
after
contractions
of
the
smaller
muscle
group.
Heart
rate
was
not
elevated
during
the
post-
exercise
occlusion
in
any
subject
for
either
form
of
contraction:
in
some
subjects,
the
heart
rate
was
slower
in
comparison
to
the
control
level
during
this
period.
438

EXERCISE
REFLEXES
DISCUSSION
In
this
study,
using
muscle
groups
of
quite
different
total
mass
and
strength,
we
have
confirmed
the
finding
of
Lind
&
McNicol
(1967)
that
the
pressor
and
heart
rate
responses
to
isometric
contractions
are
related
to
the
proportion
of
maximal
tension
achieved
rather
than
to
the
bulk
of
the
contracting
muscle
group.
The
muscular
reflex
component
of
the
stimulus
to
the
pressor
response,
however,
does
not
conform
to
this
relation:
our
experiments
in
animals
and
in
humans
indicate
that
the
muscular
reflex
drive
is
proportional
to
the
bulk
of
contracting
muscle.
The
animal
experiments
reported
here
simply
illustrated
the
inter-
actions
of
pressor
reflexes
elicited
during
muscular
contractions.
While
there
was
considerable
variability
in
the
extent
of
interaction,
all
but
two
of
our
fifteen
experiments
showed
some
additive
drive
when
the
bulk
of
contracting
muscle
was
increased,
and
this
was
so
whether
the
added
muscle
was
contracting
maximally
or
submaximally.
The
human
experi-
ments
were
a
less
direct
approach
to
the
question,
examining
the
reflex
drives
only
after
the
isometric
efforts
were
completed.
When
circulatory
occlusion
is
applied
at
the
end
of
a
period
of
contraction
induced
by
ventral
root
stimulation
in
animals,
the
pressor
response
which
is
maintained
is
not
the
full
response
which
was
achieved
during
the
contraction
(McCloskey
&
Mitchell,
1972).
This
may
mean
that
intramuscular
mechanoreceptors
contribute
part
of
the
reflex
drive
during
induced
contractions.
Such
mechanoreceptors
would
not
be
the
muscle
spindles
or
tendon
organs,
however,
as
these
have
been
shown
not
to
contribute
to
the
cardio-
respiratory
drives
in
exercise
(McCloskey
&
Mitchell,
1972;
McCloskey,
Matthews
&
Mitchell,
1972).
It
must
be
conceded
that
the
reflex
stimuli
we
investigated
in
man
were
probably
only
part
of
the
total
reflex
drive
present
during
contractions
and
that
the
value
of
the
human
experiments
is
the
confirmation
they
provide
of
the
observations
made
in
the
animal
experiments
of
this
study.
The
arguments
above
refer
only
to
the
pressor
responses
to
isometric
contractions.
In
none
of
our
experiments,
whether
in
animals
or
in
humans,
were
we
able
to
relate
the
reflex
increases
in
heart
rate
to
the
bulk
of
the
muscle
group
exercising.
This
might
lead
to
the
simple
conclusion
that
primary
muscular
reflex
effects
upon
heart
rate
are
not
related
to
the
mass
of
contracting
muscle.
While
this
conclusion
may
be
quite
correct,
it
should
be
recognized
that
other
factors
also
operate
upon
heart
rate.
In
particular,
the
baroreceptor-cardiodepressor
reflex
may
be
of
importance
here.
In
studies
in
man,
Cunningham,
Petersen,
Peto,
Pickering
&
Sleight
(1972)
showed
that
the
baroreflex
is
reset
and
its
sensitivity
reduced
during
isometric
handgrips,
but
that
the
sensitivity
is
substantially
439

D.
I.
McCLOSKEY
AND
K.
A.
STREATFEILD
restored
during
periods
of
post-exercise
occlusion.
We
have
found
also
that
in
isometric
hind-limb
contractions
induced
by
ventral
root
stimulation
in
the
dog
the
baroreceptor-cardiodepressor
reflex
is
reset,
but
we
found
no
evi-
dence
that
its
sensitivity
is
reduced
(K.
A.
Streatfeild
&
D.
I.
McCloskey,
un-
published
observations).
These
observations
open
the
following
possibilities.
During
a
voluntary
isometric
effort
the
heart
rate
rises
partly
because
the
baroreflex
sensitivity
is
reduced
(presumably
the
sensitivity
is
reduced
by
some
factor
operating
during
voluntary
contractions,
but
not
during
the
post-exercise
occlusion
period,
nor
during
induced
contractions
in
animals).
When
the
isometric
effort
is
concluded,
the
baroreflex
regains
a
great
deal,
or
all,
of
its
sensitivity
so
that
if
a
pressor
response
is
maintained,
then
the
heart
rate
is
slowed
by
the
baroreceptor
reflex.
This
would
explain
why
the
heart
rates
during
the
periods
of
post-
exercise
occlusion
were
often
slower
than
the
control
heart
rates
in
this
study
and
in
the
experiments
of
Cunningham
et
al.
(1972).
While
there
is
a
powerful
primary
cardio-acceleratory
reflex
set
up
in
the
exercising
muscle,
its
effects
are
often
wholly
or
partly
masked
by
the
baroreceptor
reflex.
Our
conclusions
regarding
the
influence
of
muscle
mass
on
heart
rate
must
therefore
be
much
less
definite
than
those
regarding
the
pressor
responses.
In
view
of
our
results
there
is
now
an
apparent
paradox.
The
pressor
response
to
a
voluntary
isometric
effort
is
related
to
the
proportion
of
maximal
tension
achieved,
and
not
to the
mass
of
muscle
contracting,
but
the
muscular
reflex
component
of
the
stimulus
for
the
pressor
response
is
related
to
the
mass
of
muscle
contracting.
If
one
were
to
believe
that
the
total
stimulus
in
exercise
is
the
simple
sum
of
contributing
stimuli,
one
would
be
forced
to
the
conclusion
that
pressor
stimuli
other
than
those
of
a
muscular
reflex
kind
are
inversely
related
to
the
bulk
of
muscle
involved
in
a
contraction.
This
is
a
conclusion
which
we
find
unattractive.
There
is
no
reason
to
assume
that
the
cardiovascular
stimuli
in
exercise
simply
summate
to
produce
their
effects.
It
is
possible
that
a
considerable
element
of
occlusion
exists.
Irradiation
of
the
central
command
is
an
important
cardiovascular
stimulus
in
exercise
(Goodwin
et
at.
1972),
and
its
inter-
action
with
the
muscular
reflex
stimulus
may
be
of
a
largely
occlusive
kind.
Present
knowledge
would
be
accounted
for
if
the
effective
cardiovascular
stimulus
were
whichever
one
of
irradiation
or
muscular
reflex
was
the
greater,
and
if
the
potency
of
irradiation
as
a
stimulus
were
related
to
the
proportion
of
maximal
effort
attained.
This
work
was
supported
by
a
grant
from
the
National
Heart
Foundation
of
Australia.
440

EXERCISE
REFLEXES41
REFERENCES
ALAM,
M.
&
SMIRK,
F.
H.
(1937).
Observations
in
man
upon
a
blood
pressure
raising
reflex
arising
from
the
voluntary
muscles.
J.
Physiol.
89,
372-383.
BROWN,
M.
C.,
LAWRENCE,
D.
G.
&
MATTHEWS,
P.
B.
C.
(1969).
Static
fusimotor
fibres
and
the
position
sensitivity
of
muscle
spindle
receptors.
Brain
Res.
14,
173-187.
COOTE,
J.
H.,
HILTON,
S.
M.
&
PEREZ-GONZALEZ,
J.
F.
(1971).
The
reflex
nature
of
the
pressor
response
to
muscular
exercise.
J.
Physiol.
215,
789-804.
CUINNINGHAM,
D.
J.
C.,
STRANGE
PETERSEN,
E.,
PETO,
R.,
PICKERING,
T.
G.
&
SLEIGHT,
P.
(1972).
Comparison
of
the
effect
of
different
types
of
exercise
on
the
baroreflex
regulation
of
heart
rate.
Acta
physiol.
scand.
86,
444-455.
GOODWIN,
G.
M.,
MCCLOSKEY,
D.
I.
&
MITCHELL,
J.
H.
(1972).
Cardiovascular
and
respiratory
responses
to
changes
in
central
command
during
isometric
exercise
at
constant
muscle
tension.
J. Physiol.
226,
173-190.
HUMPHREYS,
P.
W.
&
LIwD,
A.
R.
(1963).
Blood
flow
through
active
and
inactive
muscles
of
the
forearm
during
sustained
handgrip
contractions.
J.
Physiol.
166,
120-135.
LIND,
A.
R.
&
MCNICOL,
G.
W.
(1967).
Circulatory
responses
to
sustained
hand-
grip
contractions
performed
during
other
exercise,
both
rhythmic
and
static.
J.
Physiol
192,
595-607.
LIND,
A.
R.,
TAYLOR,
S.
H.,
HuImPHREYS,
P.
W.,
KENNELLY,
B.
M.
&
DONALD,
K.
W.
(1964).
The
circulatory
effects
of
sustained
voluntary
muscle
contraction.
COlin.
Sci.
27,
229-244.
MCCLOSKEY,
D.
I.,
MATTHEWS,
P.
B.
C.
&
MITCHELL,
J.
H.
(1972).
Absence
of
appreciable
cardiovascular
and
respiratory
responses
to
muscle
vibration
in
the
car.
J.
apple.
Physiol.
33,
623-628.
MCCLOSKEY,
D.
I.
&
MITCHELL,
J.
H.
(1972).
Reflex
cardiovascular
and
respiratory
responses
originating
in
exercising
muscle.
J.
Physiol.
224,
173-186.
441
