
Office of Behavioral and Social Sciences Research
Strategic Plan 1997
by
Norman B. Anderson, Ph.D
U.S. Department of Health and Human Services
National Institutes of Health
Office of Behavioral and Social Sciences Research
Publication Number 97-4237

TABLE OF CONTENTS
Foreword...........................................................................................Page 4
Preface..........................................................................................,...Page 5
Section One: Introduction...............................................................Page 6
The Need for Behavioral and Social Sciences Research at the National Institutes of Health
Mandates and Responsibilities of the OBSSR
The Philosophy of, and a Vision for the OBSSR
The Strategic Planning Process
Overview of the Strategic Plan
Section Two: The OBSSR Strategic Plan.......................................Page 14
Goal 1: Enhance behavioral and social sciences research and training
• Capitalize on scientic opportunities in behavioral and social research across NIH
• Enhance behavioral and social research in the NIH Intramural Research Program
• Increase training opportunities in behavioral and social sciences research
• Highlight the contributions of behavioral and social sciences research to the
improvement of health
• Increase the visibility of behavioral and social sciences within the NIH community
Goal 2: Integrate a biobehavioral interdisciplinary perspective into all NIH research area
• Increase communication and cooperation between sociobehavioral and biomedical re
searchers
• Increase inter-disciplinary training opportunities
• Create interdisciplinary funding initiatives
• Increase the visibility of behavioral and social sciences within the NIH community
Page 2

Goal 3: Improve communication among scientists and with the public
• Establish communication links between OBSSR and the behavioral and social
sciences community
• Disseminate behavioral and social science research ndings to the public and to practi-
tioners
• Improve media coverage
• Increase communications and cooperation between sociobehavioral and biomedical
researchers
• Increase visibility of behavioral and social sciences within the NIH community
Section Three: Appendices..........................................................Page 22
Appendix A: OBSSR STRATEGIC PLANNING MEETING ORGANIZING COMMITTEE
Appendix B: PARTICIPANTS IN OBSSR STRATEGIC PLANNING MEETINGS
Page 3

Forward
In 1993, the United States Congress established the Office
of Behavioral and Social Sciences Research (OBSSR) at the
National Institutes of Health (NIH). The NIH has a long history of
funding health-related behavioral and social sciences research,
and the results of this work have contributed signicantly to our
understanding, treatment, and prevention of disease. Indeed,
much of our recognition of the health risks associated with
smoking, physical inactivity, alcohol and drug abuse, poverty,
and unhealthy diets is the result of NIH-funded research.
The establishment of the OBSSR furthers the ability of the
NIH to capitalize on the scientic opportunities that exist in
behavioral and social sciences research, thereby increasing
the effectiveness of the NIH as a whole. In addition, the office
provides a focal point for the coordination of trans-NIH activities
on health and behavior.
The OBSSR officially opened on July 1, 1995, following my
appointment of Dr. Norman Anderson as its rst director. In its
two years of operation, the office has effectively highlighted the
intellectual excitement and scientic opportunities that exist in
behavioral and social sciences research and has emphasized
its potential to advance public health. Because the office is
relatively new to the NIH, it is important for it to have a blueprint
for accomplishing its goals. The strategic plan outlined in this
document provides such a blueprint, and should help to ensure
the continued success of the office.
I would like to express my sincere thanks to the OBSSR, and
to the scientists and administrators who worked to develop this
plan.
Harold E. Varmus, M.D.
Former Director, 1993-1999
National Institutes of Health
Page 4
Preface
As the rst Director of the Office of Behavioral and Social
Sciences Research (OBSSR) at the National Institutes of
Health (NIH), it is my pleasure to present the rst OBSSR
Strategic Plan. This plan is designed to guide the office’s
activities for the next three to ve years. The development
of this plan was a multifaceted process, initiated by two
meetings in February and March of 1996 with over 70
scientists and administrators. These meetings generated
hundreds of recommendations that were reviewed and
consolidated by the OBSSR staff, from which a draft plan
was developed. This draft was then sent for comment to
the governing boards of over 20 scientic societies, and
to the NIH Behavioral and Social Sciences Coordinating
Committee. Finally, the plan was then revised based on the
comments of these groups.
I would like to express my appreciation to the many
scientists and administrators who participated in our
strategic planning meetings, and whose work is reected
in this document (see list of participants at the appendix).
I would also like to thank the OBSSR staff for its diligence
throughout this process, and our consultants, John Bryson
and Charles Finn, whose expertise in strategic planning
was critical to the success of this initiative.
Norman B. Anderson, Ph.D
Founding Director, 1995-2000
Office of Behavioral and Social Sciences Research
August 1997
Page 5

Section One: Introduction
Norman B. Anderson, Ph.D.
Director, Office of Behavioral and Social Sciences Research
and Associate Director, National Institutes of Health
1. We need to
identify new behav-
ioral and social risk
factors.
The Need for Behavioral and Social Sciences Research
at the National Institutes of Health
The mission of the National Institutes of Health (NIH) is to fund and
conduct research that will improve the health of the public. Congress es-
tablished the Office of Behavioral and Social Sciences Research (OBSSR)
at the NIH to facilitate the growth and development of these important
elds. The creation of the OBSSR was in part a recognition that behavioral
and social factors are not only signicant contributors to health and illness,
but frequently interact with biological factors to inuence health outcomes.
In addition, it was recognized that behavioral and social factors represent
important avenues for treatment and prevention.
To further the mission of the NIH, four areas of behavioral and social
sciences research must be expanded.
1. We need to identify new behavioral and social risk factors for disease.
Behavioral and social sciences research funded by the NIH has contribut-
ed to the discovery of such well-known risk factors as cigarette smoking,
high-fat diets, physical inactivity, substance abuse, low socioeconomic
status and many others. Yet, there are unquestionably other behavioral and
social potential risk factors for illness that await discovery.
Page 6

3. We must develop
new behavioral and
social treatment
and prevention ap-
proaches.
4. We need more
basic behavioral
and social sciences
research.
2. We need more
research on
biological, behavior-
al, and social
interactions. We
need more research
on biological, be-
havioral, and social
interactions.
2. We need more research on biological, behavioral, and social interactions
as they affect health. It has already been discovered, for example, that
psychological stress can impair brain development, elevate blood pressure,
suppress immune system functioning, and contribute to coronary occlusion.
The hallmark of research on biopsychosocial interactions has been interdis-
ciplinary collaboration, and these efforts must be expanded.
3. We must develop new behavioral and social treatment and prevention
approaches. Directing more attention to such approaches will allow us to
continue on the remarkable progress that has already occurred in the treat-
ment and prevention of an array of disorders such as depression, heart
disease, chronic pain, infant mortality, and AIDS.
4. We need more basic behavioral and social sciences research to acceler-
ate advances in such areas as learning and memory, emotion, motivation,
perception, cognition, social class, social relations, family processes, and
cultural practices. Such research is the foundation for all other behavioral
and social sciences research.
Page 7

Mandates and Responsibilities of OBSSR
The OBSSR officially opened on July 1, 1995. The major responsibilities of the office and its
director, as mandated by Congress, may be summarized as follows:
• to provide leadership and direction in the development, renement, and implementation of
a trans-NIH plan to increase the scope of and support for behavioral and social sciences
research;
• to inform and advise the director of NIH and other key officials of trends and developments
having signicant bearing on the missions of the NIH, Department of Health and Human
Services, and other Federal agencies;
• to serve as the principal NIH spokesperson regarding research on the importance of behav-
ioral, social, and lifestyle factors in the initiation, treatment, and prevention of disease; and
to advise and consult on these topics with NIH scientists and others within and outside the
Federal Government;
• to develop a standard denition of “behavioral and social sciences research,” assess the
current levels of NIH support for this research, and develop an overall strategy for the uniform
expansion and integration of these disciplines across NIH institutes and centers;
• to promote cross-cutting, interdisciplinary research, and to integrate a biobehavioral perspec-
tive into research on the promotion of good health, and the prevention, treatment, and cure of
diseases;
• to develop initiatives designed to stimulate research in the behavioral and social sciences;
• to ensure that ndings from behavioral and social sciences research are disseminated to the
public;
• to sponsor seminars, symposia, workshops, and conferences at the NIH and at national and
international scientic meetings on state-of-the-art behavioral and social sciences research.
Page 8
The Philosophy of, and a Vision for the OBSSR
The guiding philosophy of OBSSR is that scientic advances in the understanding, treatment,
and prevention of disease will be accelerated by greater attention to behavioral and social factors
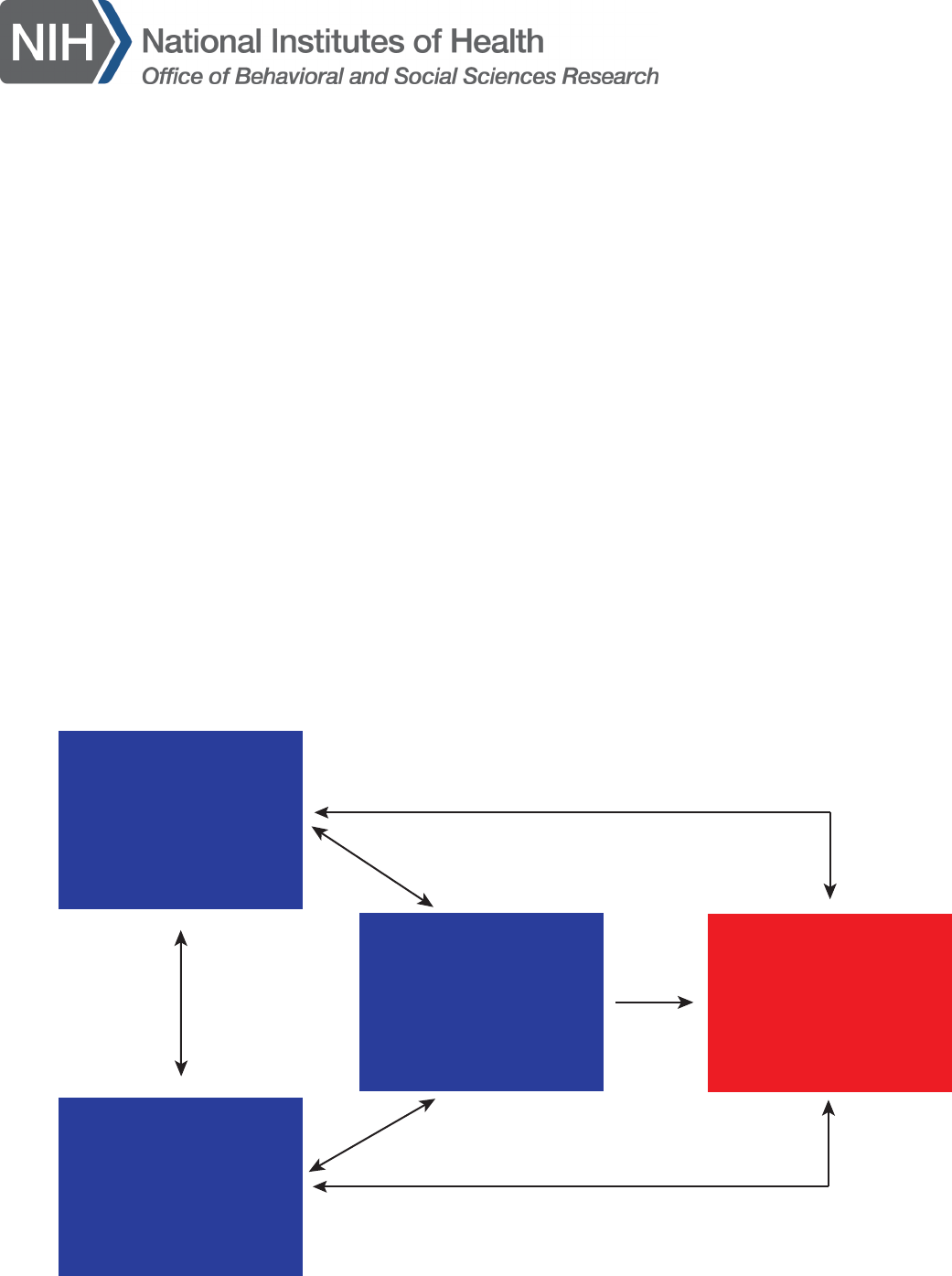
and their interaction with biomedical variables. Figure 1 illustrates the various factors that deter-
mine health outcomes, which involve behavioral/sociocultural/environmental, physiological, and
genetic factors, and the interactions among these categories. Although the contribution of each
category may vary from disease to disease, there is now ample evidence supporting this integrat-
ed perspective of causation for most health problems. For example, this conceptualization may
be applied to an array of disorders including heart disease, cancer, diabetes, AIDS, depression,
substance abuse, stroke, asthma, injuries, anxiety disorders, chronic pain, infant mortality, and
dental problems. Furthermore, the categories outlined in gure 1 represent not only risk factors
for disease, but identify targets for intervention. Although most of our treatment research efforts
have been aimed at the physiological category and associated drug interventions, research
clearly demonstrates the efficacy of behavioral and social interventions for a large number of dis-
orders. Therefore, a vision for the OBSSR is that through its work, this broader conceptualization
of health will be used to guide the scientic mission of the NIH.
behavioral,
sociocultural
and
environmental
factors
physiological
factors
health
outcomes
genetic
factors
Figure 1: Factors affecting health
Page 9

The Strategic Planning Process
In order to fulll this vision, OBSSR, during its rst year, initiated a strategic planning process.
The goal of the strategic planning process was to bring together the relevant scientic communi-
ties to assist OBSSR in charting its future direction and in establishing its priorities. Two strategic
planning meetings were held in February and March of 1996 involving over 70 scientists, science
administrators, and representatives of science organizations. These individuals worked to outline
the specic goals, strategies, and actions that are summarized in this strategic plan, which will
constitute the core activities for OBSSR over the next 3 to 5 years.
Overview of the Strategic Plan
As shown in gure 2, the ultimate objective for the NIH is to
improve health through the support of scientic research. To
achieve this objective, OBSSR will work to enhance the effec-
tiveness of the NIH through greater attention to behavioral and
social sciences research (gure 2). The OBSSR strategic plan is
organized around goals, strategies, and actions. Three goals were
improve health and
well being of people
enhance the
effectiveness of NIH
through greater attention
to behavioral and social
sciences research
identied for OBSSR and are shown in gure 3. These goals form
the core of the OBSSR strategic plan and are described on the
following pages.
Figure 2: The ultimate
objectives of the OBSSR
Page 10

improve health and
well being of people
enhance the
effectiveness of NIH
through greater attention
to behavioral and social
sciences research
enhance
behavioral and
social sciences research
and training
integrate a
biobehavioral
perspective
across NIH
improve
communications
among health
scientists and with
the public
Figure 2: The goals of the OBSSR
Goal 1
Enhance behavioral and social sciences research and training
A major part of the Congressional mandate for OBSSR was for it to work to increase support for
behavioral and social sciences research and training at NIH, both in the extramural and intramu-
ral programs. To accomplish this, OBSSR must assist NIH in identifying and capitalizing on the
numerous scientic opportunities that exist in the behavioral and social sciences. In addition to
biobehavioral research (see Goal 2 below), these opportunities exist in such areas as the iden-
tication of new risk factors; the development of new treatment and prevention approaches; and
research on basic behavioral and social processes relevant to health. The office must also work to
increase the pool of scientists who are trained to make discoveries in these areas for the ultimate
benet of the public.
Page 11

Goal 2
Integrate a biobehavioral, interdisciplinary perspective across NIH
Congress mandated that specic attention be devoted to integrating a biobehavioral perspec-
tive into research at NIH. Biobehavioral research, also known as biosocial and biopsychosocial
research, combines knowledge and approaches from biomedical, behavioral, and social science
disciplines to gain a better understanding of the complex, multifaceted interactions that deter-
mine healthy and pathological human functioning. As such, biobehavioral research represents
an exciting new frontier for the health sciences and for NIH. Examples of biobehavioral research
include such areas as behavioral cardiology, cognitive and behavioral neuroscience, psychoneuro-
immunology, and behavioral genetics.
Goal 3
Improve communication among health scientists and with the public
Improved communication among health scientists, and between scientists and the public, is
crucial to advancing behavioral and social sciences research and improving health. It was recom-
mended that OBSSR develop a comprehensive communications plan that would involve activities
aimed at 1) improving communication and information exchange among behavioral and social
scientists; 2) improving communication between sociobehavioral and biomedical scientists; 3)
increasing the dissemination of behavioral and social science ndings to the public and to health
care providers; 4) improving media coverage of behavioral and social sciences research; and 5)
ensuring that policymakers are kept abreast of developments in these elds.
Page 12

goal 1
strategy 1 strategy 2
action 1 action 2
action 3
Figure 4: The relationship between goals. strategies and actions
To achieve the three preceding goals, specic strategies and actions were recommended. Figure
4 shows the relationship between goals, strategies, and actions. The strategies represent answers
to the “what” question. That is, given the goals of OBSSR, what, in a broad sense, can the office
do to achieve them? Once broad strategies are outlined, specic actions must be delineated.
These actions represent answers to the “how’ question. That is, how do we best carry out these
strategies? Thus, actions describe the various activities that will address each strategy. In fact,
one short-term measure of the success of OBSSR, or what is often called a performance indica-
tor, is the number of recommended actions that were actually taken.
Page 13

Section Two: The OBSSR Strategic Plan
Section One: The OBSSR Strategic Plan
This section unites the OBSSR goals and strategies with specic actions. Each goal is connected
to several strategies and an even larger number of actions. The strategies and actions associat-
ed with each goal are provided below. In cases where particular actions address more than one
strategy or goal, cross-referencing is used.
Goal 1
Enhance behavioral and social sciences research and training Actions:
Strategy 1.1
1.1a Develop trans-NIH requests for applications and program announce-
ments.
Capitalize on sci-
entic opportunities
1.1b Explore partnerships between NIH institutes & centers and the private
in behavioral and
sector (e.g. managed care companies, foundations, etc.) for the funding of
social research
behavioral and social sciences research.
across NIH areas.
1.1c Use OBSSR funds to support peer-reviewed, highly rated, but
unfunded behavioral and social science proposals.
1.1d Supplement biomedical Center Grants to add behavioral and social
components (also relates to strategy 2.3).
1.1e Supplement behavioral and psychosocial treatment-related grants to
support the dissemination and implementation of ndings (also relates to
strategy 3.2).
1.1f Explore ways to expand small grant mechanisms for newer investiga-
tors.
1.1g Support conferences designed to increase interest of behavioral and
social scientists in relatively unexplored health
1.1h Provide assistance when warranted to ensure the appropriate review
of social and behavioral research grant proposals.
Page 14

Strategy 1.2
Enhance behavioral
and social research
in the NIH Intra-
mural Research
Program
Strategy 1.3
Increase training
opportunities in be-
havioral and social
sciences research
Actions
1.2a Meet with intramural research program science directors to discuss
inclusion of behavioral and social research.
1.2b Develop a postdoctoral training program for behavioral and social sci-
entists in the intramural research program (also relates to strategy 2.2).
1.2c Develop interagency personnel agreements for senior behavioral and
social scientists to work in the intramural research program (also relates to
strategies 2.2).
1.2d Send the OBSSR denition of behavioral and social sciences research
to all institute & center directors and to the NIH director explaining the
process of development of the denition and recommending that it be
adopted as the official NIH denition.
Actions
Develop postdoctoral training programs for behavioral and social scientists
in the NIH intramural research program (also relates to strategy 1.2).
Explore ways of expanding National Research Service Award support for
behavioral and social scientists.
Support short-term summer training workshops for interdisciplinary
research for social, behavioral, and biomedical scientists (also relates to
strategies 2.1 and 2.2).
Create social and behavioral science training programs for middle and high
school teachers (also relates to strategy 3.2).
Develop partnerships with foundations for funding of behavioral and social
science training.
Page 15

Strategy 1.4
Highlight the con-
tributions of be-
havioral and social
sciences research
to the improvement
of health
Strategy 1.5
Increase the visi-
bility of behavioral
and social sciences
within the NIH com-
munity
Actions
1.4a Commission literature reviews for biomedical journals on selected
topics related to behavioral and social science contributions to public health
and health science.
1.4b Develop and distribute fact sheets to relevant parties on behavioral
and social contributors to the etiology, prevention, and treatment of disease.
1.4c Develop and distribute fact sheets to relevant parties on reductions in
costs and health-care utilization resulting from behavioral and social inter-
ventions.
1.4d Identify institute & center scientic problems and provide solutions
based on behavioral and social sciences research.
1.4e Provide forums for behavioral treatment researchers to meet with
service providers (also relates to strategy 3.2).
1.4f Establish intergovernmental personnel agreements program for behav-
ioral and social science researchers to work in institute & center adminis-
trative offices.
Actions
1.5a Sponsor an ongoing scientic seminar series in conjunction with the
Behavioral and Social Sciences Research Coordinating Committee (BSSR-
CC).
1.5b Organize regular informal brieng sessions on behavioral and social
research for the NIH director and for institute & center directors.
Page 16

1.5c Facilitate behavioral and social sciences research interest groups
within the NIH community.
1.5d Organize regular conferences at NIH on cross-cutting behavioral and
social science topics.
1.5e Send the OBSSR denition of behavioral and social sciences research
to all institute & center directors and to the NIH director explaining the
process of development of the denition and recommending that it be
adopted as the official NIH denition.
Goal 2
Integrate a biobehavioral interdisciplinary perspective into all NIH research areas Actions
Strategy 2.1
Increase commu-
nication and coop-
eration between
sociobehavioral
and biomedical
researchers
2.1a Sponsor workshops, speakers, and symposia at NIH and at profes-
sional meetings on interdisciplinary research for behavioral and biomedical
investigators.
2.1b Commission literature reviews for biomedical publications that inte-
grate and highlight biobehavioral interactions (also relates to strategy 1.4).
2.1c Develop cross-disciplinary funding initiatives (also relates to strategy
2.3).
2.1d Create an internet-based discussion group for cross-disciplinary ex-
changes.
2.1e Establish a working group to promote cross-disciplinary research.
2.1f Convene a consensus conference on a common nomenclature for
“phases” of behavioral treatment research, analogous to that used for
clinical trials in medical studies, to facilitate communication and under-
standing across biomedical and behavioral treatment areas.
2.1g Establish intergovernmental personnel agreements program for extra-
mural behavioral and social scientists to work at NIH (also relates to strate-
gies 1.2 and 1. 4 ).
Page 17

Strategy 2.2
Increase
inter-disciplinary
training opportuni-
ties
Strategy 2.3
Create
inter-disciplinary
funding initiatives
Actions
2.2a. Support short-term training workshops for biomedical and behavioral
scientists to become familiar with each others’ methods and procedures
(also relates to strategy 1.3).
2.2b. Conduct behavioral and social science research methodology work-
shops at biomedical meetings (also relates to strategy 1.3).
2.2c. Develop post-doctoral fellowship program in the NIH intramural
research program (also relates to strategies 1.2, 1.3, 2.4).
2.2d. Enlist the assistance of the Institute of Medicine of the National
Academy of Sciences in examining training requirements for interdisciplin-
ary research (also relates to strategy 1.3).
Actions
2.3a. Supplement biomedical research centers with funds for interdisciplin-
ary pilot research (also relates to strategy 1.1).
2.3b. Develop trans-NIH requests for applications and program announce-
ments that require interdisciplinary collaborations (also relates to strategy
1. 1 ).
2.3c. Supplement biomedical requests for applications and program an-
nouncements to support biobehavioral research (also relates to strategy
1. 1 ).
Page 18

Strategy 2.4
(see strategy 1.5 for specic actions)
Increase the
visibility of behav-
ioral and social
sciences within the
NIH community
Goal 3
Improve communication among scientists and with the public Actions:
Strategy 3.2
Disseminate
behavioral and
social science
research ndings
to the public and to
practitioners
Actions
3.2a. Improve media coverage of behavioral research (also relates to
strategy 3.3).
3.2b. Create a website for lay audiences summarizing new ndings.
3.2c. Provide forums for clinical researchers to meet with service providers
(also relates to strategy 1.4).
3.2d. Assist in the development of clinical guidelines for the use of behav-
ioral treatment approaches.
3.2e. Develop funding initiatives on dissemination of behavioral and social
science research ndings (also relates to strategy 1.1).
3.2f. Hold periodic briengs for Congressional members and staffers on
important ndings in the behavioral and social sciences.
3.2g. Write Opinion/Editorial articles on ndings relevant to current issues
in public health (also relates to strategy 3.3).
3.2h. Work with health care providers and managed care companies to
incorporate scientically validated behavioral treatment approaches into
medical care.
Page 19

Strategy 3.3
Improve media
coverage
3.2i. Conduct lectures for patient advocacy groups.
3.2j. Create social and behavioral science training programs for middle and
high school teachers (also relates to strategy 1.3).
3.2k. Create programs that encourage researchers to guest lecture in local
community.
3.2l. Meet regularly with representatives from behavioral and social science
organizations and their boards of directors.
3.2m. Organize workshops on how behavioral and social scientists can
involve and get the support of local communities for research.
Actions
3.3a. Assess the current status of behavioral and social science research
coverage in the print media.
3.3b. Organize a series of seminars for medical and science writers on
important new ndings.
3.3c. Invite media representatives to visit active sociobehavioral laborato-
ries and eld sites.
3.3d. Provide information on new ndings in the behavioral and social
sciences to NIH public affairs and communications offices.
3.3e. Co-sponsor science writer fellowships in conjunction with science
organizations.
3.3f. Write Opinion/Editorial pieces on social and behavioral research
relevant to current public health issues (also relates to strategy 3.2).
3.3g. Develop and distribute one-page fact sheets to media representatives
on the relevance of behavioral and social factors to the etiology, prevention,
and treatment of disease (also relates to strategy 1.4).
Page 20


Section Three: Appendices
Appendix A:
OBSSR STRATEGIC PLANNING MEETING ORGANIZING COMMITTEE
Ronald Abeles, Ph.D.
Behavioral and Social Research Program
National Institute on Aging
National Institutes of Health
Bethesda, MD
Edward Laumann, Ph.D.
Sociology Department
University of Chicago
Chicago, IL
Lucile Adams-Campbell, Ph.D.
Howard University Cancer Center
Washington, DC
Barbara Rimer, Ph.D.
Duke Comprehensive Cancer Center
Duke University School of Medicine
Durham, NC
Norman B. Anderson, Ph.D.
Office of Behavioral and Social Sciences Research
Office of the Director
National Institutes of Health
Bethesda, MD
Susan Solomon, Ph.D.
Office of Behavioral
and Social Sciences Research
Office of the Director
National Institutes of Health
Bethesda, MD
Virginia Cain, Ph.D.
Office of Behavioral
and Social Sciences Research
Office of the Director
National Institutes of Health
Bethesda, MD
Marina L. Volkov, Ph.D.
Office of Behavioral
and Social Sciences Research
Office of the Director
National Institutes of Health
Bethesda, MD
Margaret Chesney, Ph.D.
Prevention Sciences Group
School of Medicine
University of California, San Francisco
San Francisco, CA
Ellen Stover, Ph.D.
Office on AIDS
National Institute of Mental Health
National Institutes of Health
Rockville, MD
James Jackson, Ph.D.
Institute for Social Research
University of Michigan
Ann Arbor, MI
Consultants
John Bryson, Ph.D.
Minneapolis, MN
Charles Finn
Minneapolis, MN
Page 22

Appendix B:
PARTICIPANTS IN OBBSR STRATEGIC PLANNING MEETINGS
Ronald Abeles, Ph.D.
Behavioral and Social Research Program
National Institute on Aging
National Institutes of Health
Bethesda, MD
Hortensia Amaro, Ph.D.
Department of Social and Behavioral Sciences
School of Public Health
University of Boston
Boston, MA
Norman B. Anderson, Ph.D.
Office of Behavioraland Social Sciences Research
Office of the Director
National Institutes of Health
Bethesda, MD
Judith Auerbach, Ph.D.
Office of AIDS Research
Office of the Director
National Institutes of Health
Bethesda, MD
Frank Baker
American Cancer Society
Atlanta, GA
Wendy Baldwin, Ph.D.
Office for Extramural Research
Office of the Director
National Institutes of Health
Bethesda, MD
Gordon Bower, Ph.D.
Condence Training, Inc.
Stanford, CA
Kelly Brownell, Ph.D.
Department of Psychology
Yale University
New Haven, CT
Virginia Cain, Ph.D.
Office of Behavioral
and Social Sciences Research
Office of the Director
National Institutes of Health
Bethesda, MD
Patricia Carpenter, Ph.D.
Department of Psychology
Carnegie Mellon University
Pittsburgh, PA
Margaret Chesney, Ph.D.
Prevention Sciences Group
School of Medicine
University of California, San Francisco
San Francisco, CA
Rodney R. Cocking, Ph.D.
National Research Council
Washington, DC
R. Lorraine Collins, Ph.D.
Research Institute on Addictions
Buffalo, NY
Rena Convissor, M.P.H.
Center for the Advancement of Health
Washington, DC
Paul Costa, Ph.D.
Laboratory of Personality and Cognition
National Institute on Aging
National Institutes of Health
Baltimore, MD
Cynthia Costallo, Ph.D.
American Sociological Association
Washington, DC
Page 23

Joel Dimsdale, M.D.
Department of Psychiatry
University of Southern California
La Jolla, CA
Glen Elder, Ph.D.
Carolina Population Center
University of North Carolina, Chapel Hill
Chapel Hill, NC
John A. Fairbank, Ph.D.
Research Triangle Institute
Research Triangle Park, NC
Representing International Society for
Traumatic Stress Studies
Geraldine Felton, Ed.D., R.N., F.A.A.N.
College of Nursing
University of Iowa
Iowa City, IA
Richard Fuller, M.D.
Division of Clinical
and Prevention Research
National Institute on Alcohol Abuse
and Alcoholism
National Institutes of Health
Rockville, MD
Thomas Glynn, Ph.D.
Division of Cancer Prevention
and Control
National Cancer Institute
National Institutes of Health
Rockville, MD
Ellen Gritz, Ph.D.
Department of Behavioral Sciences
M.D. Anderson Cancer Center
Houston, TX
Linda Harootyan
Gerontological Society of America
Washington, DC
Christine R. Hartel, Ph.D.
American Psychological Association
Washington, DC
Ed Hatcher
American Sociological Association
Washington, DC
Laura Hayman, Ph.D., R.N.
School of Nursing and Medicine
University of Pennsylvania
Wyndmoor, PA
Representing the American Heart Association
Loretta Sweet Jemmott, Ph.D., R.N.
School of Nursing
University of Pennsylvania
Philadelphia, PA
David Johnson, Ph.D.
Federation of Behavioral, Psychological
and Cognitive Sciences
Washington, DC
Ernest Johnson, Ph.D.
Department of Family Medicine
Morehouse School of Medicine
Atlanta, GA
Joyce Justus, Ph.D.
Office of Science and Technology Policy
The White House
Washington, DC
Peter Kaufmann, Ph.D.
Division of Epidemiology
and Clinical Applications
National Heart, Lung, and Blood Institute
National Institutes of Health
Rockville, MD
Page 24

Patricia C. Kobor
American Psychological Association
Washington, DC
Norman Krasnegor, Ph.D.
Center for Research
on Mothers and Children
National Institute of Child Health
and Human Development
National Institutes of Health
Rockville, MD
Alan Kraut, Ph.D.
American Psychological Society
Washington, DC
John Lanigan, Jr., Ph.D.
Institute for the Advancement
of Social Work Research
Washington, DC
Edward Laumann, Ph.D.
Sociology Department
University of Chicago
Chicago, IL
Eleanor Maccoby, Ph.D.
Department of Psychology
Stanford University
Stanford, CA
George Maddox, Ph.D.
Center for Study of Aging
and Human Development
Duke University Medical Center
Durham, NC
Karen Matthews, Ph.D.
Department of Psychiatry
University of Pittsburgh
Pittsburgh, PA
Sandra J. McElhaney, M.A.
National Mental Health Association
Alexandria, VA
John McKinlay, Ph.D.
New England Research Institute
Watertown, MA
Kristin Moore, Ph.D.
Child Trends
Washington, DC
Representing the Population Association
of America
Judith Ockene, Ph.D.
Division of Preventive
and Behavioral Medicine
University of Massachusetts
Medical School
Worcester, MA
Mary Margaret Overbey, Ph.D.
American Anthropological Association
Arlington, VA
Mary Ellen Oliveri, Ph.D.
Division of Neuroscience
and Behavioral Science
National Institute of Mental Health
National Institutes of Health
Rockville, MD
C. Tracy Orleans, Ph.D.
Research and Evaluation Division
The Robert Wood Johnson Foundation
Princeton, NJ
Susan Persons
Society for Research
on Child Development
Washington, DC
Thomas Pickering, M.D., Ph.D.
Cornell Medical Center
New York, NY
Representing the Academy of Behavioral
Medicine Research
Page 25

Harold Pincus, M.D.
American Psychiatric Association
Washington, DC
Stephen W. Porges, Ph.D.
University of Maryland
College Park, MD
Representing the Society for
Psychophysiological Research
Enola Proctor, Ph.D.
George Warren Brown School
of Social Work
Washington University
St. Louis, MO
Gary Sandefur, Ph.D.
Department of Sociology
University of Wisconsin - Madison
Madison, WI
Julia R. Scott, R.N.
National Black Womens’ Health Project
Washington, DC
Angela L. Sharpe
Consortium of Social Science Associations
Washington, DC
Paula Skedsvold, Ph.D.
Society for the Psychological
Study of Social Issues
Washington, DC
James Smith, Ph.D.
Rand Corporation
Santa Monica, CA
Susan Solomon, Ph.D.
Office of Behavioral
and Social Sciences Research
Office of the Director
National Institutes of Health
Bethesda, MD
Linda Spear, Ph.D.
Department of Psychology
State University of New York, Binghamton
Binghamton, NY
Gerald Sroufe
American Educational Research Association
Washington, DC
Sarah Evans Stevens
Federation of Behavioral, Psychological
and Cognitive Sciences
Washington, DC
Ellen Stover, Ph.D.
Office on AIDS
National Institute of Mental Health
National Institutes of Health
Rockville, MD
Tony Strickland, Ph.D.
Biobehavioral Research Center
Charles R. Drew University
of Medicine and Science
Los Angeles, CA
Stephen Suomi, Ph.D.
Laboratory of Comparative Ethology
National Institute of Child Health
and Human Development
National Institutes of Health
Bethesda, MD
Jennifer Sutton
Association of American Medical Colleges
Washington, DC
Jose Szapocznik, Ph.D.
Department of Psychiatry
and Behavioral Sciences
University of Miami School of Medicine
Miami, FL
Robert Trotter, Ph.D.
Page 26

Department of Anthropology
Northern Arizona University
Flagstaff, AZ
Jaylan Turkkan, Ph.D.
Division of Basic Research
National Institute on Drug Abuse
National Institutes of Health
Rockville, MD
Donald Vereen, Ph.D.
Office of the Director
National Institute on Drug Abuse
National Institutes of Health
Rockville, MD
Marina L. Volkov, Ph.D.
Office of Behavioral
and Social Sciences Research
Office of the Director
National Institutes of Health
Bethesda, MD
Linda Waite, Ph.D.
Department of Sociology
University of Chicago
Chicago, IL
Stephen Weiss, Ph.D., M.P.H.
Department of Psychiatry
and Behavioral Sciences
University of Miami School of Medicine
Miami, FL
redford Williams, M.D.
Department of Psychiatry
Duke University Medical School
Durham, NC
Judith Costine Woodward
Society of Behavioral Medicine
Rockville, MD
Page 27

Publication Number 97-4237
Publication Title Strategic Plan for the Office of Behavioral and Social Sciences Research at NIH
Year Published 1997
IC Office of The Director
Page 28
