
ATTITUDES AND SOCIAL COGNITION
Longevity Increased by Positive Self-Perceptions of Aging
Becca R. Levy and Martin D. Slade
Yale University
Suzanne R. Kunkel
Miami University
Stanislav V. Kasl
Yale University
This research found that older individuals with more positive self-perceptions of aging, measured up
to 23 years earlier, lived 7.5 years longer than those with less positive self-perceptions of aging. This
advantage remained after age, gender, socioeconomic status, loneliness, and functional health were
included as covariates. It was also found that this effect is partially mediated by will to live. The sample
consisted of 660 individuals aged 50 and older who participated in a community-based survey, the Ohio
Longitudinal Study of Aging and Retirement (OLSAR). By matching the OLSAR to mortality data
recently obtained from the National Death Index, the authors were able to conduct survival analyses. The
findings suggest that the self-perceptions of stigmatized groups can influence longevity.
There has been a proliferation of studies in the last 6 years
showing the effects of race and gender self-stereotypes on behav-
ior and function (e.g., Leyens, Desert, Croizet, & Darcis, 2000;
Steele & Aronson, 1995; Stone, Lynch, Sjomeling, & Darley,
1999). Most of these studies have explained their findings by
referring to stereotype threat (Wheeler & Petty, 2001). Essentially,
this theory states that members of stigmatized groups “experience
stereotype threat when they are in situations in which other people
may view them stereotypically in ways likely to increase perfor-
mance pressures” (Blasovich, Spencer, Quinn, & Steele, 2001, p.
225). According to the theory, “susceptibility to stereotype threat
lies not in the internalization of the stereotype, but in caring about
the domains to which it might prove to be a frustration” (Crocker,
Major, & Steele, 1998, p. 519).
Self-stereotypes of aging, or older individuals’ beliefs about old
people as a category, do not appear to fit into the stereotype-threat
framework. The underlying reason is that self-stereotypes of aging
seem to develop and operate through internalization. We believe
older individuals’ internalized age stereotypes contribute to the
formation of their self-perceptions of aging, which, in turn, can
have a physiological outcome. In this study, we partially address
this model by examining whether self-perceptions of aging influ-
ence survival.
Unlike race and gender stereotypes, which individuals encounter
while developing group self-identities, individuals acquire age
stereotypes several decades before becoming old. Thus, younger
individuals are likely to automatically accept age stereotypes with-
out questioning their validity (Nelson, 2002; Perdue & Gurtman,
1990). When individuals reach old age and the stereotypes become
self-relevant, they have already internalized these stereotypes
(Giles, Fox, & Smith, 1993; Levy & Langer, 1994).
Once individuals become older, they may lack the defenses of
other groups to ward off the impact of negative stereotypes on
self-perceptions. For example, African Americans are potentially
able to defend themselves against stereotype threat by disengaging
from the academic domain (Steele & Aronson, 1995). This with-
drawal is facilitated by the stipulation that stereotype threat arises
in specific situations, under specific conditions, when one is en-
gaging in specific tasks (e.g., Steele & Aronson, 1995).
An equivalent disengagement is less likely to be an option for
older individuals because the central themes of self-stereotypes of
aging are health and function or their absence, which promotes a
diffusiveness that transcends domains (Levy, Hausdorff, Hencke,
& Wei, 2000). The all-encompassing nature of self-stereotypes of
aging may not lend itself to disengagement for older individuals in
the same way as, for instance, academic stereotypes do for African
Becca R. Levy, Martin D. Slade, and Stanislav V. Kasl, Department of
Epidemiology and Public Health, Yale University; Suzanne R. Kunkel,
Scripps Gerontology Center, Miami University.
Martin D. Slade is now at the Department of Biostatistics, Harvard
University.
This research was generously supported by a fellowship from the
Brookdale Foundation and by a National Institute on Aging grant
(AG05727) to Becca R. Levy. We thank Heiner Maier for his helpful
comments.
Correspondence concerning this article should be addressed to Becca R.
Levy, Department of Epidemiology and Public Health, Yale University,
P.O. Box 208034, 60 College Street, New Haven, Connecticut 06520-
Journal of Personality and Social Psychology, 2002, Vol. 83, No. 2, 261–270
Copyright 2002 by the American Psychological Association, Inc. 0022-3514/02/$5.00 DOI: 10.1037//0022-3514.83.2.261
261
Americans or employment stereotypes do for women. The diffu-
siveness of age stereotypes can be seen in a series of laboratory
studies demonstrating that the same sets of positive and negative
primes, typified by wise versus senile, can lead to enhancement or
decline, respectively, in a wide array of cognitive and behavioral
outcomes, including memory performance, handwriting, self-
efficacy, mathematical performance, and views of other older
people (Levy, 1996; Levy et al., 2000).
The depth and breadth of self-stereotypes of aging may be
explained by their focus on cognitive and physical decline, which
conveys a sense of the ultimate outcome: death (Becker, 1980;
Levy et al., 1999–2000). This outcome does not facilitate com-
partmentalization into a domain: “The knowledge of the inevita-
bility of death is the underlying sense from which all other fears
are ultimately derived” (McCoy, Pyszczynski, Solomon, & Green-
berg, 2000, p. 37).
A second self-protective strategy practiced by other stigmatized
groups that may be less accessible for older individuals is egali-
tarian thinking. Controlled personal beliefs are capable of inhibit-
ing the earlier-developed negative stereotypes toward women and
African Americans by asserting later-acquired egalitarianism (De-
vine, 1989; Devine & Monteith, 1999). However, egalitarianism,
as promoted by the women’s, civil rights, and political correctness
movements, does not exist to the same degree in relation to age
stereotypes as it does for gender and race stereotypes (Levy &
Banaji, 2002). There is, then, a greater likelihood that younger
individuals will accept negative stereotypes about aging as true
and that this will continue to occur when the individuals become
older and the stereotypes become self-stereotypes. This acceptance
diminishes the prospect for defending self-perceptions against
negative age stereotypes.
There are two additional indications that aging self-stereotypes
are internalized. First, research suggests that self-stereotypes of
aging can operate without older individuals’ awareness. This is in
contrast to the noninternalization that characterizes stereotype
threat and is reflected in its reliance on awareness at critical stages:
recognition that a stereotype may be applied to oneself in a
particular situation and that one may then act in accordance with it
(e.g., Crocker et al., 1998).
The series of laboratory studies that achieved cognitive and
physical changes in older participants did so by flashing aging
stereotype primes on a screen at a speed that was below the
threshold of awareness (see Levy, 1996, for a more detailed
description of the procedure). In one of the studies, older individ-
uals who were first exposed to subliminal negative age stereotype
primes and then to cognitive challenges showed a significantly
heightened cardiovascular response, compared with those exposed
to subliminal positive age stereotypes and the same challenges. Yet
the two groups of older individuals did not differ in how stressful
they rated the challenges to be (Levy et al., 2000). There was, then,
unawareness not only of the stereotype primes but also of their
physiological impact.
Another study showed that the same subliminal priming of age
stereotypes can influence a behavior that is thought to operate
largely without awareness: handwriting (Allport & Vernon, 1933;
Wolff, 1948). A panel of judges who did not know the age and
priming group of the older participants described handwriting
samples from the negatively primed group as significantly deteri-
orated, compared with baseline, whereas those participants who
received positive primes were rated as significantly more accom-
plished (Levy, 2000).
A further indication that self-stereotypes of aging are internal-
ized is that older individuals tend to hold feelings toward their own
group that are as negative as the feelings held about it by those
outside their group—the young (Nosek, Banaji, & Greenwald,
2002). Similarly, older individuals are more likely to oppose
programs that benefit the aged than are younger individuals (Levy
& Shlesinger, 2001; Shlesinger & Kronebusch, 1994). This con-
trasts with the in-group preference of other stigmatized groups
(Levy & Banaji, 2002). For instance, Asians and African Ameri-
cans, in spite of acknowledging that they are perceived in negative
terms, tend to hold as positive views toward their respective groups
as Whites do toward their own group (Crocker et al., 1998).
Although the writings of the Symbolic Interactionists are re-
garded as inconsistent with stereotype-threat theory (Crocker et al.,
1998), these writings help to explain the process by which self-
stereotypes of aging are internalized and affect self-perceptions of
aging. These scholars, including Charles Horton Cooley and
George Herbert Mead, conceptualized the self as a product of
societal beliefs conveyed through social interaction (Cooley, 1902;
Mead, 1934). Such beliefs are likely to include both the positive
and the negative age stereotypes that exist in American culture
(Brewer, Dull, & Lui, 1981; Hummert, 1999) rather than only the
negative stereotypes that are addressed by stereotype threat (e.g.,
Steele & Aronson, 1995). Studies of older individuals have found
a correspondence between self-stereotypes and self-perceptions
(Imamoglu, Kueller, Imamoglu, & Kueller, 1993; Levy, 1999).
The preponderance of negative aging stereotypes in society does
not guarantee a preponderance of internalized negative aging ste-
reotypes, nor of eventual negative aging self-perceptions. Within
the elderly category, subgroups may have different exposures to
aging stereotypes. As an example, older Deaf individuals report
more positive attitudes toward aging than do older individuals who
are not hearing impaired (Levy & Langer, 1994). Older members
of the Deaf community tend to participate in intergenerational
activities, in which they are given equal or higher status, to a
greater extent than do older hearing individuals (Becker, 1980);
this type of intergenerational contact may be a source of insulation
from mainstream negative stereotypes.
Further, among those who are exposed to the same stereotypes
within the same subgroups, there is variability in what is internal-
ized. For instance, older role models can provide young individ-
uals with a countervailing force against negative stereotypes of
aging (Palmore, 1998). In addition, personality differences may
affect receptivity to stereotypes (Allport, 1954).
Link Between Self-Perception of Aging and Longevity
Most of the research on self-stereotypes and self-perceptions
referred to here has been confined to the laboratory, which un-
avoidably imposes limitations. There is no way of knowing
whether the stimuli and paradigms authentically represent how
self-stereotypes and self-perceptions operate in the real world and
over time. In the present research, we partially address these
limitations by examining, in the community, the impact of aging
self-perceptions on a long-term outcome: longevity.
The lengthening of the average American life span by 27 years
over the last century has provoked considerable research on the
262
LEVY, SLADE, KUNKEL, AND KASL
determinants of longevity (e.g., Perls & Silver, 1999; Rogers,
Hummer, & Nam, 2000). Much of this research has focused on
genes (e.g., Pletcher, Houle, & Curtsinger, 1999; Rogina, Reenan,
Nilsen, & Helfand, 2000). Yet as much as 75% of longevity may
be due to nongenetic attributes, including psychological and be-
havioral factors (Vaupel et al., 1998). In addition, most of the
research on predictors of survival has focused on negative factors
(e.g., disease, injury, and cognitive decline; Stroebe, 2000). Rela-
tively few studies have examined positive factors, such as benefi-
cial beliefs, that might affect survival. The following study exam-
ines for the first time whether positive self-perceptions about one’s
aging influence survival, controlling for functional health and
other relevant factors.
We have located only one other study that considered the link
between views of aging and survival. In the Berlin Aging Study,
researchers examined the association between 17 indicators of
psychological functioning and mortality during 7 years in a sample
that was 70 years or older (Maier & Smith, 1999). The authors did
not expect views of aging to emerge as a significant predictor. Yet,
after systematically inspecting the variables, they found that one of
the best predictors of mortality was the Attitude Toward Own
Aging subscale of the Philadelphia Geriatric Center Morale Scale
(PGCMS; Lawton, 1975; Liang & Bollen, 1983), controlling for
age, socioeconomic status, life satisfaction, self-rated health, num-
ber of illnesses, and cognition. Partially because of the lack of a
functional health variable in their analyses, the authors concluded
that the negative beliefs about aging are “probably not the cause
for an increased mortality risk, but they may reflect potential
causes from other domains of functioning” (Maier & Smith, 1999,
p. 51). By contrast, our study, which includes functional health as
a covariate, is designed to explore the possibility that self-
perceptions of aging directly affect survival.
Overview
In the following two studies, we examine whether self-
perceptions of aging influence longevity and how this process
might occur. We conducted our analyses by matching data from
the Ohio Longitudinal Study of Aging and Retirement (OLSAR)
with data from the National Death Index (NDI).
The OLSAR serves our research aims because it (a) contains
items at baseline that measured self-perceptions of aging; (b)
allows us to chart the course of survival over a 22.6-year period;
(c) includes individuals, 50 years old or more, who are at the
threshold of aging, thus allowing us to explore the reach of aging
self-perceptions; and (d) contains survey waves, collected after
baseline, that allow us to examine a psychological mechanism by
which aging self-perceptions might influence longevity.
Study 1
In the first study, after controlling for relevant factors, we
examined the hypothesis that those with more positive aging
self-perceptions at baseline will live longer.
Method
Participants
In 1975, Robert Atchley and his colleagues at Miami University re-
cruited participants for the OLSAR in Oxford, Ohio. Because of the small
size of the town (a population of approximately 15,000), the investigators
were able to contact virtually all individuals who met the participation
criteria of being (a) cognitively intact, (b) age 50 or over by July 1, 1975,
and (c) a community resident. The investigators compiled the list of
potential participants by starting with the voter registration records and
then using a variety of other techniques, including a postcard census of all
mailing addresses in the community, a review of welfare rolls, and com-
munity informants. The efforts to recruit all eligible individuals in the town
maximized the heterogeneity of the sample characteristics as well as the
variability in beliefs about aging. The study team identified a total of 1,461
eligible individuals, of whom 1,157 participated.
We added two criteria for inclusion of participants in the analyses. They
had to (a) meet the vital-status protocol (included in the Measures section,
within the description of the survival variable) and (b) provide complete
data for the variables analyzed in the study. We excluded 139 participants
because they did not meet the vital-status protocol and another 358 par-
ticipants because they were missing data for at least one of the variables.
A total of 660 participants met these additional inclusion criteria.
The final cohort comprised 338 men and 322 women. Their age at
baseline ranged from 50 to 94 years (M ⫽ 63.00 years, SD ⫽ 9.23). Their
mean score on the Health Scale for the Aged (Rosow & Breslau, 1966)
was 4.84 (the items for this scale are listed under Covariates in the
Measures section). Scores on the Health Score for the Aged ranged from 0
to 6, with a higher score reflecting better health. The participants’ average
socioeconomic status, as measured by the Two-Factor Index of Social
Position (Hollingshead, 1965), was 32.49, which indicates that participants
tended to be middle class. Scores on this scale ranged from 11, indicating
the highest socioeconomic status, to 77, indicating the lowest socioeco-
nomic status.
The final cohort of 660 participants did not differ from the excluded
participants in age, socioeconomic status, or functional health. However,
the final cohort significantly differed by gender and race. In the total
sample of individuals recruited, 42.7% were male, as opposed to 51.2% in
the final cohort. Also, in the total sample of individuals recruited, 4.6%
were Black or “other,” whereas 2.5% described themselves as Black or
“other” in the final cohort.
Measures
Independent variable: Self-perceptions of aging. For our self-
perceptions of aging measure, we used the Attitudes Toward Own Aging
subscale that Liang and Bollen (1983) based on five items from the
PGCMS (Lawton, 1975). This subscale consists of the following items:
“Things keep getting worse as I get older,”“I have as much pep as I did
last year,”“As you get older, you are less useful,”“I am as happy now as
I was when I was younger,” and “As I get older, things are (better, worse,
or the same) as [sic] I thought they would be.”
Participants responded to the first four items with a “no,” scored as 0, or
“yes,” scored as 1. The first and third items were reverse scored to make
all the items measure a positive aging self-perception. As indicated, par-
ticipants responded to the fifth item by selecting either “better,”“worse,”
or “the same.” To make the fifth item comparable to the other four items,
we changed it to a dichotomous variable and combined “the same” re-
sponses with “worse” responses (in analyses presented in the Results
section, we verified that combining “the same” responses with “better”
responses did not change the impact of the independent variable on
survival). Participants received a total score ranging from 0 to 5, with a
higher score indicating a more positive aging self-perception.
Several researchers found that these five items loaded highly on a single
factor in different data sets (Liang & Bollen, 1983; Mancini, Shade, &
Quinn, 1995; McCulloch, 1991). We conducted a factor analysis to check
that the items also loaded on one factor in the OLSAR. Indeed, when we
conducted a factor analysis with all the PGCMS items, the five items
loaded on a single factor with all factor loadings greater than .40, thus
meeting the definition of meaningful loadings (Hatcher, 1994). These five
263
LONGEVITY FROM POSITIVE SELF-PERCEPTIONS

PGCMS items had not previously been examined as a subscale in the
OLSAR.
Outcome: Survival. Our outcome variable is survival. This is the first
study to match the OLSAR with mortality data, which we obtained from
the NDI.
For the analyses, we used the number of days participants survived after
the baseline interview. The survival variable ranged from the baseline
survey in 1975 to January 1, 1998, the cut-off date for mortality data
available from the NDI. To determine whether and when participants had
died, we developed a vital-status protocol on the basis of information
provided by the NDI, which included possible matches of deceased indi-
viduals on three variables: first and last name; date of birth; and state in
which death occurred, as most of the cohort did not move out of Ohio
before death. To be considered dead, participants needed to match on all
three criteria (264, or 43%, of the participants coded as dead were in this
group) or match on two of the three criteria and have confirmation by an
obituary and/or an informant (355, or 57%, of the participants coded as
dead were in this group). If the OLSAR participants only matched the NDI
data by date of birth and state in which death occurred, to be considered
dead they also had to match on first name (some of the participants
changed their last name with marriage or divorce).
To be considered alive, participants were (a) confirmed to be living
through January 1, 1998, by the participants themselves; (b) confirmed to
be living through January 1, 1998, by an informant and had no matches
provided by the NDI (368, or 92%, of the participants coded as alive were
in either this group or the first group); or (c) had one match provided by the
NDI but also sent in a survey response after the NDI date of death (31, or
8%, of the participants coded as alive were in this group).
Covariates. The covariates for this study include the following mea-
sures assessed at baseline: age; gender; race, as categorized by either White
or Black or “other”; and socioeconomic status (Hollingshead, 1965), which
takes into account participants’ years of education and occupational status.
Baseline functional health was also included as a covariate. It was
assessed by Rosow and Breslau’s (1966) six-item Health Scale for the
Aged. Participants were asked,
Which of the following things are you physically able to do? (Place a
check by each of the things you can do): 1. heavy work around the
house (shoveling snow, washing walls, etc.); 2. work at a full time
job; 3. ordinary work around the house; 4. walk half a mile; 5. go out
to a movie, to church, to a meeting or to visit friends or relatives; 6.
walk up and down stairs.
Each check was scored as a 1. Thus, the scores ranged from 0 to 6, with
a lower score indicating lower functional health. We analyzed this measure
as an ordinal variable. Others have found that the Health Scale for the Aged
strongly correlates with observed physical performance measures (Alex-
ander et al., 2000).
In addition, we included two covariates that could be alternative expla-
nations for self-perceptions of aging influencing survival: self-rated health
and loneliness. There is considerable evidence that self-rated health influ-
ences survival (Idler & Kasl, 1992; Idler, Russell, & Davis, 2000). It has
been shown that loneliness predicts survival and tends to correlate with
another predictor of survival: depression (for which there was no OLSAR
measure; Cacioppo et al., 2000; Danner, Snowdon, & Friesen, 2001; Dill
& Anderson, 1999). By adding self-rated health and loneliness as covari-
ates, we tried to make sure that self-perceptions of aging is a new explan-
atory variable and not just another way to measure more established
variables.
We measured self-rated health by the item “Is your health improving,
declining or remaining about the same?” Loneliness was measured by the
PGCMS item “How much do you feel lonely?” with not much scored as 1
and a lot scored as 2 (Lawton, 1975).
Statistical Analyses
To examine whether more positive aging self-perceptions at baseline
lead to greater longevity after relevant factors are controlled for, we used
univariate and multivariate Cox proportional-hazards regression models.
The regression models used days since baseline interview as the time scale.
The analyses were conducted in stages. First, we conducted two Kaplan–
Meier survival curves: one with each value of the self-perception of aging
measure examined separately, and one with the participants dichotomized
into those below and those equal to or above the self-perception of aging
mean of 3.67 (see Figure 1).
Figure 1. Influence of positive self-perceptions of aging (PSPA) on survival. Arrow indicates median survival.
264
LEVY, SLADE, KUNKEL, AND KASL

Next, we conducted several tests of the assumptions for proportional
hazards, such as visual inspection of log-log survival curves and inclusion
of a Self-Perception of Aging ⫻ Log (Time) interaction term in the model.
For all of these tests as well as all additional analyses reported, the
self-perceptions of aging measure was analyzed as a continuous variable.
These tests indicated that the assumptions for proportional hazards were
met by the data.
Then, after analyzing the self-perceptions of aging risk ratio using a
univariate Cox proportional-hazards regression model, we added the fol-
lowing potential covariates to our model: age at baseline, race, gender,
socioeconomic status, functional health, self-rated health, and loneliness.
Using a backward-elimination strategy, we reduced covariates to those
significant at .05. Before eliminating nonsignificant covariates, we checked
that their removal did not produce a meaningful change (greater than 1%)
in the self-perceptions of aging hazard ratio. The final multivariate model
therefore contained only those control variables that significantly predicted
survival and/or confounded the relationship between self-perceptions and
survival (see Table 1). Accordingly, race and self-rated health were
eliminated.
Results
The results support the hypothesis of Study 1: Those with more
positive aging self-perceptions at baseline live longer, after rele-
vant factors are controlled for.
In the initial analysis, before the covariates were added, those
with more positive self-perceptions of aging scores survived sig-
nificantly longer than did those with more negative self-
perceptions of aging scores. When we conducted a Kaplan–Meier
survival analysis with self-perceptions of aging as a dichotomous
variable, we found that the median survival of those in the more
positive self-perceptions of aging group was 7.6 years longer than
the median survival of those in the more negative aging self-
stereotype group (see Figure 1). That is, the median survival for
the more positive self-perceptions group was 22.6 years past
baseline, whereas the median survival for those in the more neg-
ative self-perceptions group was 15 years. Using the nonparamet-
ric log-rank test, we found that the two groups were significantly
different (p ⬍ .001). When we conducted a Cox proportional-
hazards regression model with self-perceptions of aging as a
continuous variable, each one-point increase in self-perceptions of
aging showed a consistent increase in survival.
The influence of sequentially adding covariates to the model on
the positive self-perceptions of aging survival risk ratio is pre-
sented in Table 1. The final survival model, with all the covariates
added, is presented in the extreme right column.
When the self-perceptions of aging score acted as a predictor,
the survival risk ratio remained significant after we sequentially
adjusted for covariates. The risk ratio of .87 (p ⬍ .001) suggests
that positive self-perceptions of aging reduce the risk of mortality.
For each change of one point in the positive self-perception of
aging measure, the risk of dying decreased by 13%. When we ran
the model with the PGCMS item “As I get older, things are (better,
worse, or the same) as [sic] I thought they would be” recalculated
so that “the same” was combined with “better” rather than with
“worse,” a similar result emerged: The risk ratio of positive self-
perceptions on survival became .89 (p ⬍ .004).
Ordered from greatest to least impact on survival, the variables
were in the following sequence: age, self-perceptions of aging,
gender, loneliness, functional health, and socioeconomic status.
We determined this by multiplying each variable’s coefficient by
the mean of the variable and then taking the absolute value.
Visual inspection of the data revealed that the trend of more
positive aging self-perceptions leading to greater longevity con-
sistently appeared when we repeated this analysis six times after
stratifying by age, gender, socioeconomic status, functional health,
and loneliness. That is, we divided the participants into two sets of
age groups (less than 60 years old or 60 years old and over, and
less than 70 years old or 70 years old and over), two gender
groups, two health groups (those below and those equal to or
greater than the functional health mean of 4.84), two socioeco-
nomic status groups (those below and those equal to or greater than
the socioeconomic status mean of 32.49), and groups of those who
reported they felt lonely and those who reported they did not. In all
the analyses, those with more positive self-perceptions of aging
outlived those with more negative self-perceptions of aging.
We were able to establish that the influence of self-perceptions
of aging on survival was a larger effect than the total PGCMS from
which the self-perceptions of aging measure’s items were taken.
We did this by conducting three additional survival analyses with
the PGCMS items. First, we modeled survival as a function of the
total PGCMS score, controlling for age, functional health, gender,
and socioeconomic status. The hazard ratio was .97 (p ⫽ .06; 95%
confidence interval [CI] ⫽ .94–1.00). The same analysis (see
Table 1), using the self-perceptions of aging measure, significantly
predicted survival ( p ⬍ .001). In addition, the sum of the PGCMS
items, excluding the five used for the self-perceptions of aging
measure, did not significantly predict survival when we controlled
for age, functional health, gender, and socioeconomic status (p ⫽
.38). Third, we found that self-perceptions of aging still signifi-
Table 1
Relationship Between Positive Self-Perceptions of Aging (PSPA) and Survival
Risk ratio
for
PSPA alone
Risk ratio for PSPA adjusted for:
Age Age, sex Age, sex, SES
Age, sex, SES,
functional health
Final model:
Age, sex, SES,
functional health,
loneliness
.78 .90 .88 .88 .90 .87
(0.74–0.83) (0.84–0.95) (0.83–0.94) (0.82–0.94) (0.84–0.97) (0.80–0.94)
p ⬍ .001 p ⬍ .001 p ⬍ .001 p ⬍ .001 p ⬍ .006 p ⬍ .001
Note. Confidence intervals appear in parentheses. SES ⫽ socioeconomic status.
265
LONGEVITY FROM POSITIVE SELF-PERCEPTIONS
cantly predicted survival (hazards ratio ⫽ .88, p ⫽ .008; 95% CI ⫽
.81–.97) after we controlled for the sum of the PGCMS items,
excluding the five used for the self-perceptions of aging measure,
as well as age, functional health, gender, and socioeconomic
status.
Discussion
The findings from Study 1 suggest that self-perceptions of aging
have an impact on survival—when age, functional health, gender,
and socioeconomic status are controlled for—that is greater than
the impact of some other variables that have been previously
linked to survival, including gender, socioeconomic status, func-
tional health, and loneliness. A primary question that arises from
these findings is, By what mechanism do self-perceptions influ-
ence survival? In the following study, we explore whether will to
live acts as an intervening variable.
Study 2
Our finding in Study 1, that a social–psychological variable
directly influences survival, raises the question of whether an
additional psychological mechanism might act as a mediator. On
the basis of our prior research and the research of others, we
predicted that if self-perceptions of aging affect survival, the
underlying mechanism would be, in part, through will to live (Idler
& Kasl, 1992; Levy et al., 1999–2000; Phillips & Smith, 1990;
Sinard, 2001). We define will to live as a judgment that the
perceived benefits of one’s life outweigh the perceived hardships.
One of the reasons we predicted will to live may act as a
mediator between self-perceptions of aging and survival is that
among the views of aging that are internalized from a young age
are beliefs about the inverse relationship between the value and the
length of older persons’ lives. These beliefs are reinforced
throughout a lifetime, particularly in old age. A parody of one way
these messages may be transmitted to older individuals can be
found in a cartoon depicting a doctor telling an older patient, “It
appears that you’ll definitely outlive your usefulness” (Cullum,
2001).
In a previous study, we found that views of aging can affect
older individuals’ reported will to live. When we subliminally
exposed older individuals to negative stereotypes of aging, they
were significantly more likely to reject life-prolonging medical
treatment in hypothetical scenarios, whereas those in the positive
stereotype group were significantly more likely to accept life-
prolonging medical treatments (Levy et al., 1999–2000). As pre-
dicted, this effect did not appear in the young, for whom the age
stereotypes and the outcome of will to live were not as relevant.
This age stereotype effect occurred regardless of the financial or
familial burden associated with the hypothetical medical treat-
ments (Levy et al., 1999–2000). These findings suggest that the
positive stereotypes of aging primes tilted the will-to-live balance
toward the perceived benefits of life, whereas the negative stereo-
types tilted the balance toward the perceived hardships of life.
Although we did not measure self-perceptions of aging in the
previous study, the connection between age stereotypes and will to
live suggested to us that will to live might act as mediator between
aging self-perceptions and survival.
A number of studies have generated a pattern of findings that
suggest that will to live affects survival. Although the investigators
of these studies did not directly measure will to live, this concept
is often implied. One set of studies has demonstrated that the
timing of deaths is affected by holidays. Chinese American women
are more likely to die during the week after the Harvest Moon
Festival, a holiday in which they play a prominent role, rather than
during the week before it (Phillips & Smith, 1990). Jewish men are
more likely to die immediately after than right before Passover, an
8-day holiday in which they traditionally have greater psycholog-
ical and ritual involvement than do Jewish women, for whom no
such mortality effect emerged (Idler & Kasl, 1992; Phillips &
King, 1988). Among Christians, both men and women are more
likely to die in the month following Christmas and Easter than in
the month before these holidays (Idler & Kasl, 1992).
The relationship between significant holidays and survival is not
limited to specific ethnic or religious groups. For example, one
study found a sharp increase of deaths in the month after the
much-anticipated January 1, 2000 (Sinard, 2001). The author con-
cluded that because “a likely contributing factor was desire of
patients to live into the next century...these data suggest a role
for the patient’s state of mind in postponing his or her own
outcome” (Sinard, 2001, p. 1707).
These studies suggest that the anticipation of holidays and the
holidays themselves provide a perceived benefit that is transient
insofar as it ends when the holidays do; at that point, the perceived
hardships of life become more salient than the perceived benefits.
The outcome appears to reflect a shift from will to live to what
might be called will to die. Will to die occurs when the perceived
hardships of one’s life outweigh the perceived benefits. A study of
over 1.5 million Finnish married persons, aged 35 to 84, found that
mortality is higher than normal in the first 6 months after the death
of a spouse (Martickainen & Valkonenen, 1996). The authors
attributed the finding to “an overall weakening of a persons’ ability
to resist and cope with disease” (p. 1092).
The capacity to cope with a newly imposed perceived hardship
is perhaps due to the reservoir of preexisting perceived benefits
that carry over to the new challenge. A related phenomenon was
conceptualized by Ryff and Singer (1998) as the life of purpose, or
fulfilled life, that helps individuals cope with trauma.
We were able to examine whether will to live partially mediates
the relationship between self-perceptions of aging and survival
because the OLSAR included follow-up survey waves containing
variables that we believe measure our hypothetical mediator, will
to live.
Method
Although the analyses share with Study 1 the predictor variable (self-
perceptions of aging, measured at baseline) and the outcome variable
(survival), we added our predicted mediator, will to live.
Our will-to-live measure was developed from three items appearing in a
14-item semantic differential measure that was included in the 1977 wave
of follow-up data collection. The questions were prefaced with the follow-
ing statement: “Below is a list of adjectives that can be used to describe a
person’s life. For each line, check the one box that best describes what you
think about your life in retirement.” The responses consisted of paired
words on opposite ends of a 7-point scale. The three semantic differential
items we selected included the following pairs of adjectives: empty–full,
hopeless–hopeful, and worthless–worthy. These adjectives seemed to most
266
LEVY, SLADE, KUNKEL, AND KASL
closely correspond to our earlier-stated definitions of will to die and will to
live, respectively. That is, when the perceived hardships of one’s life
outweigh the perceived benefits, we expect an outlook that is empty,
hopeless, and worthless, whereas when the perceived benefits of one’s life
outweigh the perceived hardships, we expect an outlook that is full,
hopeful, and worthy. These items loaded on a single factor, with loadings
greater than .86.
Results
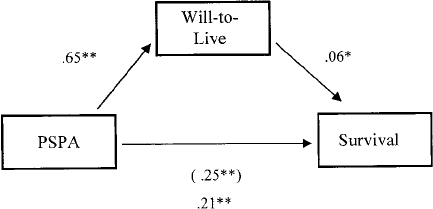
As predicted by Study 2’s hypothesis, we found that will to live
partially mediated the relationship between positive self-
perceptions of aging and survival. The will-to-live variable ful-
filled the three criteria for a partial mediator (see Figure 2; Kenny,
Kashy, & Bolger, 1998). Complying with the first criterion, we
found that the initial variable, self-perceptions of aging, predicted
the outcome of survival,

⫽ .2464, SE ⫽ .0291, p ⬍ .001. (This
is consistent with findings from Study 1.) Complying with the
second criterion, we found the initial variable, self-perceptions of
aging, correlated with the presumed mediator, will to live. That is,
when we regressed will to live on self-perceptions of aging, this
was significant (

⫽ .6458, SE ⫽ .0937, p ⬍ .001). According to
the third criterion, we found that the presumed mediator, will to
live, affected the outcome, survival, even when we controlled for
the direct path between the initial variable, self-perceptions of
aging, and the outcome, survival (

⫽ .0555, SE ⫽ .0266, p ⬍
.04). Even though the beta weight associated with the direct path
from self-perceptions of aging to survival was reduced with the
inclusion of the presumed mediator, will to live, in the model,
self-perceptions of aging still predicted survival in this final equa-
tion (

⫽ .2058, SE ⫽ .0533, p ⬍ .001). Thus, it appears that will
to live acts as a partial mediator and does not completely mediate
the relationship between baseline self-perceptions of aging and
survival. In further support that will to live acts as a partial
mediator, according to Baron and Kenny’s (1986) modification of
the Sobel test, we found that the Z score associated with will to live
as a mediator was significant (Z ⫽ 1.97, p ⬍ .03).
To increase our confidence that will to live partially mediates
the relationship between self-perceptions of aging and survival, we
conducted an additional analysis with an alternative relationship
between the variables. We examined whether it is possible that
self-perceptions of aging mediate the relationship between will to
live and survival. To check this, we repeated the mediational
analysis, but with will to live (in 1975) as the predictor and
self-perceptions of aging (in 1977) as the mediator. We found that
self-perceptions of aging did not fit the definition of a mediator
(Kenny et al., 1998). Although the first criterion was fulfilled (will
to live measured in 1975 significantly predicted survival) and the
second criterion was fulfilled (will to live measured in 1975
significantly predicted self-perceptions of aging in 1977), the third
criterion was not met. That is, self-perceptions of aging measured
in 1977 did not significantly predict survival when we controlled
for the 1975 will to live.
Discussion
As predicted, we found that will to live partially mediated the
relationship between self-perceptions of aging and survival,
whereas self-perceptions of aging did not mediate the relationship
between will to live and survival.
Our findings from Study 2 suggest that positive self-perceptions
of aging lengthened survival both directly and indirectly. Even
with the indirect path added, the direct path between self-
perceptions of aging and survival remained fairly strong. This
indicates that although will to live is part of the process by which
self-perceptions of aging influence survival, other mediators are
probably involved. Another likely means is cardiovascular re-
sponse to stress, which earlier research has shown can be adversely
affected when elderly participants are exposed to negative stereo-
types of aging (Levy et al., 2000).
The semantic differential questions of the OLSAR, on which we
based our will-to-live measure, were framed in terms of retirement.
This raises the possibility that the participants were considering the
will-to-live items specifically in terms of retirement rather than in
terms of a broader perspective. The importance of retirement as a
rite of passage was suggested by Neugarten (1996), who described
the continuum of views toward it: At one end, “many people
describe retirement as a period characterized by monotony, bore-
dom and decline, a period marking time until death”; at the other
end, life in retirement provides “time to develop new interests and
with opportunities to extend not only one’s lifetime but also what
can be called one’s personal biography”(p. 223). To examine the
role played by retirement in response to the will-to-live measure,
we compared responses of those who reported they were em-
ployed, housewives, or retired. No differences emerged between
the responses of these groups, suggesting that this measure acts as
more than a proxy for retirement. In short, however salient retire-
ment may be, will to live appears to reflect thoughts that go beyond
the participants’ job status.
General Discussion
This study found that positive self-perceptions of aging mea-
sured up to 23 years earlier contributed to individuals living
longer. The advantage remained after we controlled for age, gen-
der, socioeconomic status, loneliness, and functional health. Self-
perceptions of aging had a greater impact on survival than did
gender, socioeconomic status, loneliness, and functional health in
this cohort. The robustness of our finding is further suggested by
our demonstration that those in the more positive self-perception
of aging group demonstrated better survival among men as well as
women, those with better as well as worse functional health, those
less than 60 years as well as 60 years and over, those less than 70
Figure 2. Will to live as a partial mediator between positive self-
perceptions of aging (PSPA) and survival. The number in parentheses
indicates the direct effect of PSPA on survival prior to inclusion of the
mediator in the regression equation. * p ⬍ .05. ** p ⬍ .001.
267
LONGEVITY FROM POSITIVE SELF-PERCEPTIONS
years as well as 70 years and over, those with lower as well as
higher socioeconomic status, and those who reported experiencing
loneliness as well as those who did not.
The increased life span of 7.5 years in our study is considerable,
especially when we compare our findings with those of other
longevity studies. The effect of more positive self-perceptions of
aging on survival is greater than the physiological measures of low
systolic blood pressure and cholesterol, each of which is associated
with a longer life span of 4 years or less (Friedman et al., 1995).
The survival advantage of more positive self-perceptions of aging
is also greater than the independent contribution of lower body
mass index, no history of smoking, and a tendency to exercise;
each of these factors has been found to contribute between 1 and 3
years of added life (Fraser & Shavlik, 2001).
Our self-perceptions of aging measure provided a partial inven-
tory of the participants’ definition of their old age. Because we
assume that these definitions tend to evolve, in part, from the age
stereotypes internalized in childhood and beyond, they are unlikely
to be consciously evaluated (Levy & Banaji, 2002). Nevertheless,
self-perceptions of aging are likely to generate feelings of benefit
or hardship that we suggest are evaluated within the mediating
phase that constitutes the will to live. Hence, we found that the
more positive the self-perceptions of aging were, the greater was
the will to live, and this partially mediated the relationship between
self-perceptions of aging and survival.
Even though there are, as noted in the introduction, important
differences between the old and other targeted groups, our findings
demonstrate that the old cannot be considered in monolithic terms.
As an example, although the old may lack certain defenses against
internalizing negative stereotypes of aging, our data show that a
considerable number of individuals are able to successfully cope
with these stereotypes.
Additionally, although the theory of stereotype threat excludes
internalization and therefore sets it apart from self-stereotypes of
aging, this does not preclude the possibility that racism is inter-
nalized by its targets. Indeed, studies using a scale designed to
measure the internalized racism of African Americans have found
an association between this variable and a number of psycholog-
ical and behavioral outcomes (Taylor, Henderson, & Jackson,
1991; Williams & Williams-Morris, 2000). Also, an association
has been found among African Americans between accepting the
validity of racist stereotypes and chronic health problems (Wil-
liams & Chung, in press). For many chronic illnesses, African
Americans have a higher mortality rate than do Whites (Rogers et
al., 2000).
It is, therefore, possible to propose that a fundamental common-
ality may arise from the impact of stigmatization. Although further
exploration is needed, our study suggests that the process shared
by stigmatized groups may be found in the effect of self-
stereotypes on self-perceptions. To the extent that the process is
shared, there is a greater likelihood that the outcome will be as
well. Accordingly, our study carries two messages. The discour-
aging one is that negative self-perceptions can diminish life ex-
pectancy; the encouraging one is that positive self-perceptions can
prolong life expectancy.
There is clearly a need to ameliorate the discouraging message.
One approach would emphasize positive stereotypes of aging
among the young by such means as promoting positive intergen-
erational activities. Another approach would deemphasize negative
stereotypes of aging by, for instance, encouraging older individu-
als to monitor the correspondence between the ways they are
targeted by others and the ways they target themselves. An incen-
tive for engaging in this process of self-awareness might follow
from a recognition that stigmatization can carry with it the ultimate
penalty.
However, both these approaches are piecemeal measures. If a
previously unidentified virus was found to diminish life expect-
ancy by over 7 years, considerable effort would probably be
devoted to identifying the cause and implementing a remedy. In
the present case, one of the likely causes is known: societally
sanctioned denigration of the aged. A comprehensive remedy
requires that the denigrating views and actions directed at elderly
targets undergo delegitimization by the same society that has been
generating them.
References
Alexander, N. B., Guire, K. E., Thelen, D. G., Ashton-Miller, J. A.,
Schultz, A. B., Grunawalt, J. C., & Giordani, B. (2000). Self-reported
walking ability predicts functional mobility performance in frail
older adults. Journal of the American Geriatrics Society, 48, 1408–
1413.
Allport, G. (1954). The nature of prejudice. Cambridge, MA: Addison-
Wesley.
Allport, G., & Vernon, P. (1933). Studies in expressive movement. New
York: Macmillan.
Baron, R. M., & Kenny, D. A. (1986). The moderator–mediator variable
distinction in social psychological research: Conceptual, strategic, and
statistical considerations. Journal of Personality and Social Psychol-
ogy, 51, 1173–1182.
Becker, E. (1980). The denial of death. New York: Macmillan.
Blasovich, J., Spencer, S. J., Quinn, D., & Steele, C. (2001). African
Americans and high blood pressure: The role of stereotype threat.
Psychological Science, 12, 225–229.
Brewer, M. B., Dull, V., & Lui, L. (1981). Perceptions of the elderly:
Stereotypes as prototypes. Journal of Personality and Social Psychol-
ogy, 41, 656–670.
Cacioppo, J. T., Ernst, J. M., Burleson, M. H., McClintock, M. K.,
Malarkey, W. B., Hawkley, L. C., et al. (2000). Lonely traits and
concomitant physiological processes: The MacArthur social neuro-
science studies. International Journal of Psychophysiology, 35, 143–
154.
Cooley, C. H. (1902). Human nature and the social order. New York:
Scribner.
Crocker, J., Major, B., & Steele, C. (1998). Social stigma. In D. T. Gilbert,
S. T. Fiske, & G. Lindzey (Eds.), The handbook of social psychology
(pp. 504–553). New York: McGraw-Hill.
Cullum, L. (2001, July 16). It appears that you’ll definitely outlive your
usefulness [cartoon]. New Yorker, p. 69.
Danner, D. D., Snowdon, D. A., & Friesen, W. V. (2001). Positive
emotions in early life and longevity: Findings from the Nun Study.
Journal of Personality and Social Psychology, 80, 804–813.
Devine, P. G. (1989). Stereotypes and prejudice: Their automatic and
controlled components. Journal of Personality and Social Psychol-
ogy, 56, 5–18.
Devine, P. G., & Monteith, M. J. (1999). Automaticity and control in
stereotyping. In S. Chaiken & Y. Trope (Eds.), Dual-process theories in
social psychology (pp. 339–360). New York: Guilford Press.
Dill, J. C., & Anderson, C. A. (1999). Loneliness, shyness, and depression:
The etiology and interrelationships of everyday problems in living. In T.
Joiner & J. C. Coyne (Eds.), The interactional nature of depression:
268
LEVY, SLADE, KUNKEL, AND KASL
Advances in interpersonal approaches (pp. 93–125). Washington, DC:
American Psychological Association.
Fraser, G. E., & Shavlik, D. J. (2001). Ten years of life: Is it a matter of
choice? Archives of Internal Medicine, 161, 1645–1652.
Friedman, H. S., Tucker, J. S., Schwartz, J. E., Tomlinson-Keasey, C.,
Martin, L. R., Wingard, D. L., & Criqui, M. H. (1995). Psychosocial and
behavioral predictors of longevity. American Psychologist, 50, 68–78.
Giles, H., Fox, S., & Smith, E. (1993). Patronizing the elderly: Intergen-
erational evaluations. Research on Language & Social Interaction, 26,
129–149.
Hatcher, L. (1994). A step-by-step approach to using the SAS system for
factor analysis and structural equation modeling. Cary, NC: SAS Insti-
tute.
Hollingshead, A. B. (1965). Two factor index of social position. Unpub-
lished manuscript, Yale University.
Hummert, M. L. (1999). A social cognitive perspective on age stereotypes.
In T. M. Hess & F. Blanchard-Fields (Eds.), Social cognition and aging
(pp. 175–196). New York: Academic Press.
Idler, E. L., & Kasl, S. V. (1992). Religion, disability, depression, and the
timing of death. American Journal of Sociology, 97, 1052–1079.
Idler, E. L., Russell, L. B., & Davis D. (2000). Survival, functional
limitations, and self-rated health in the NHANES I Epidemiologic
Follow-up Study, 1992. First National Health and Nutrition Examination
Survey. American Journal of Epidemiology, 152, 874–883.
Imamoglu, E. O., Kueller, R., Imamoglu, V., & Kueller, M. (1993). The
social psychological worlds of Swedes and Turks in and around retire-
ment. Journal of Cross-Cultural Psychology, 24, 26–41.
Kenny, D. A., Kashy, D. A., & Bolger, N. (1998). Data analysis in social
psychology. In D. T. Gilbert, S. T. Fiske, & G. Lindzey (Eds.), The
handbook of social psychology (pp. 233–265). New York: McGraw-Hill.
Lawton, M. P. (1975). The Philadelphia Geriatric Center Morale Scale: A
revision. Journal of Gerontology, 30, 85–89.
Levy, B. (1996). Improving memory in old age by implicit self-
stereotyping. Journal of Personality and Social Psychology, 71, 1092–
1107.
Levy, B. R. (1999). The inner self of the Japanese elderly: A defense
against negative stereotypes of aging. International Journal of Aging
and Human Development, 48, 131–144.
Levy, B. R. (2000). Handwriting as a reflection of aging self-stereotypes.
Journal of Geriatric Psychiatry: A Multidisciplinary Journal of Mental
Health and Aging, 33, 81–94.
Levy, B. R., Ashman, O., & Dror, I. (1999–2000). To be or not to be: The
effects of aging self-stereotypes on the will-to-live. Omega: Journal of
Death and Dying, 40, 409–420.
Levy, B. R., & Banaji, M. R. (2002). Implicit ageism. In T. Nelson (Ed.),
Ageism: Stereotypes and prejudice against older persons (pp. 49–75).
Cambridge: MIT Press.
Levy, B. R., Hausdorff, J., Hencke, R., & Wei, J. Y. (2000). Reducing
cardiovascular stress with positive self-stereotypes of aging. Journals of
Gerontology: Psychological Sciences, 55, 205–213.
Levy, B. R., & Langer, E. J. (1994). Aging free from negative stereotypes:
Successful memory among the American Deaf and in China. Journal of
Personality and Social Psychology, 66, 935–943.
Levy, B. R., & Shlesinger, M. (2001, November). Impact of age stereo-
types on older individuals’ rejection of elderly-benefiting policies. Paper
presented at the annual meeting of the Gerontological Society of Amer-
ica, Chicago, IL.
Leyens, J.-P., Desert, M., Croizet, J.-C., & Darcis, C. (2000). Stereotype
threat: Are lower status and history of stigmatization preconditions of
stereotype threat? Personality and Social Psychology Bulletin, 26,
1189–1199.
Liang J., & Bollen K. A. (1983). The structure of the Philadelphia Geriatric
Center Morale Scale: A reinterpretation. Journal of Gerontology, 38,
181–189.
Maier, H., & Smith, J. (1999). Psychological predictors of mortality in old
age. Journals of Gerontology: Psychological Sciences, 54, 44–54.
Mancini, J. A., Shade, D. D., & Quinn, W. H. (1995). Measuring morale:
Note on use of factor scores. Psychological Reports, 56, 139–144.
Martickainen, P., & Valkonenen, T. (1996). Mortality after the death of
spouse: Rates and causes of death in a large Finnish cohort. American
Journal of Public Health, 86, 1087–1093.
McCoy, S. K., Pyszczynski, T., Solomon, S., & Greenberg, J. (2000).
Transcending the self: A terror management perspective on successful
aging. In A. Tomer (Ed.), Death attitudes and the older adult (pp.
37–63). Philadelphia: Brunner-Routledge.
McCulloch, J. B. (1991). A longitudinal investigation of the factor struc-
ture of subjective well-being: The case of the Philadelphia Geriatric
Center Morale Scale. Journals of Gerontology: Psychological Sci-
ence, 46, 251–258.
Mead, G. H. (1934). Mind, self and society. Chicago: University of Chi-
cago Press.
Nelson, T. (Ed.). (2002). Ageism: Stereotypes and prejudice against older
persons. Cambridge, MA: MIT Press.
Neugarten, D. A. (1996). The meaning of age. Selected papers of Bernice
Neugarten. Chicago: University of Chicago Press.
Nosek, B. A., Banaji, M. R., & Greenwald, A. G. (2002). Harvesting
implicit group attitudes and beliefs from a demonstration website. Group
Dynamics, 6, 101–115.
Palmore, E. B. (1998). The facts on aging quiz. New York: Springer.
Perdue, C. W., & Gurtman, M. B. (1990). Evidence for the automaticity of
ageism. Journal of Experimental Social Psychology, 26, 199–216.
Perls, T. T., & Silver, M. H. (1999). Living to 100: Lessons in living to your
maximum potential at any age. New York: Basic Books.
Phillips, D. P., & King, E. W. (1988). Death takes a holiday: Mortality
surrounding major social occasions. Lancet, 2, 728–732.
Phillips, D. P., & Smith, D. G. (1990). Postponement of death until
symbolically meaningful occasions. Journal of the American Medical
Association, 263, 1947–1951.
Pletcher S. D., Houle, D., & Curtsinger, J. W. (1999). The evolution of
age-specific mortality in Drosophila melanogaster: Genetic divergence
among unselected lines. Genetics, 153, 813–823.
Rogers, R. G., Hummer, R. A., & Nam, C. B. (2000). Living and dying in
the USA: Behavioral, health, and social differentials of adult mortality.
New York: Academic Press.
Rogina, B., Reenan, R. A., Nilsen, S. P., & Helfand, S. L. (2000). Extended
life-span conferred by cotransporter gene mutations in Drosophila. Sci-
ence, 290, 2137–2140.
Rosow, I., & Breslau, N. (1966). A Guttman health scale for the aged.
Journal of Gerontology, 21, 556–559.
Ryff, C. D., & Singer, B. (1998). The contours of positive human health.
Psychological Inquiry, 9, 1–28.
Shlesinger, M., & Kronebusch, K. (1994). Intergenerational tensions and
conflict: Attitudes and perceptions about social justice and age-related
needs. In V. L. Bengston & R. A. Harootyan (Eds.), Intergenerational
linkages: Hidden connections in American society (pp. 152–184). New
York: Springer.
Sinard, J. H. (2001). Y2K revisited: A human component? Journal of the
American Medical Association, 285, 1706–1707.
Steele, C. M., & Aronson, J. (1995). Stereotype threat and the intellectual
test performance of African Americans. Journal of Personality and
Social Psychology, 69, 797–811.
Stone, J., Lynch, C. I., Sjomeling, M., & Darley, J. M. (1999). Stereotype
threat effects on black and white athletic performance. Journal of Per-
sonality and Social Psychology, 77, 1213–1227.
Stroebe, W. (2000). Social psychology and health. Philadelphia: Open
University Press.
Taylor, J., Henderson, D., & Jackson, B. B. (1991). A holistic model for
269
LONGEVITY FROM POSITIVE SELF-PERCEPTIONS

understanding and predicting depression in African American women.
Journal of Community Psychology, 19, 306–320.
Vaupel, J. W., Carey, J. R., Christensen, K., Johnson, T. E., Yashin, A. I.,
Holm, N. V., et al. (1998). Biodemographic trajectories of longevity.
Science, 280, 855–860.
Wheeler, S. C., & Petty, R. E. (2001). The effects of stereotype activation
on behavior: A review of possible mechanisms. Psychological Bulletin,
127, 797–826.
Williams, D. R., & Chung, A. (in press). Racism and health. In R. Gibson
& J. S. Jackson (Eds.), Health in Black America. Thousand Oaks, CA:
Sage.
Williams, D. R., & Williams-Morris, R. (2000). Racism and mental health:
The African American experience. Ethnicity and Health, 5, 243–268.
Wolff, W. (1948). Diagrams of the unconscious: Handwriting and per-
sonality in measurement, experiment and analysis. New York: Grune &
Stratton.
Received November 13, 2000
Revision received January 8, 2002
Accepted January 8, 2002 䡲
270
LEVY, SLADE, KUNKEL, AND KASL
